Zeng Zhu, Yang Biao, Liao Zhengyin
Department of Abdominal Oncology, West China Medical School, West China Hospital, Sichuan University, Chengdu, China.
Department of Gastroenterology, West China Hospital, West China Medical School, Sichuan University, Chengdu, China.
Front Oncol. 2021 Mar 11;11:650481. doi: 10.3389/fonc.2021.650481. eCollection 2021.
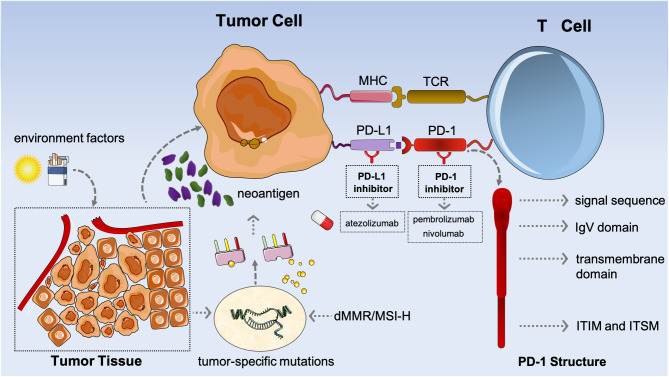
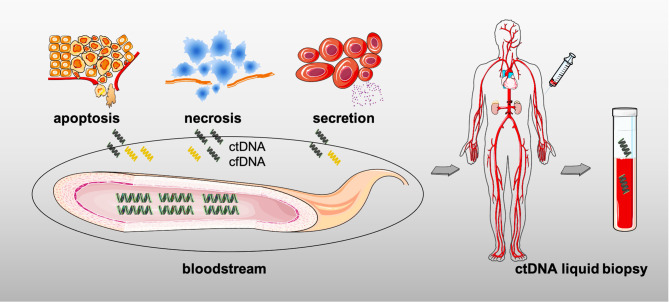
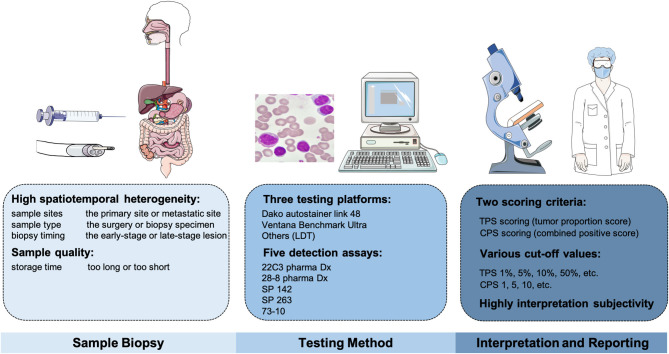
Immunotherapy, represented by immune checkpoint inhibitors (mainly referring to programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) blockades), derives durable remission and survival benefits for multiple tumor types including digestive system tumors [gastric cancer (GC), colorectal cancer (CRC), and hepatocellular carcinoma (HCC)], particularly those with metastatic or recurrent lesions. Even so, not all patients would respond well to anti-programmed death-1/programmed death-ligand 1 agents (anti-PD-1/PD-L1) in gastrointestinal malignancies, suggesting the need for biomarkers to identify the responders and non-responders, as well as to predict the clinical outcomes. PD-L1expression has increasingly emerged as a potential biomarker when predicting the immunotherapy-based efficacy; but regrettably, PD-L1 alone is not sufficient to differentiate patients. Other molecules, such as tumor mutational burden (TMB), microsatellite instability (MSI), and circulating tumor DNA (ctDNA) as well, are involved in further explorations. Overall, there are not still no perfect or well-established biomarkers in immunotherapy for digestive system tumors at present as a result of the inherent limitations, especially for HCC. Standardizing and harmonizing the assessments of existing biomarkers, and meanwhile, switching to other novel biomarkers are presumably wise and feasible.
以免疫检查点抑制剂(主要指程序性死亡蛋白1(PD-1)/程序性死亡配体1(PD-L1)阻断剂)为代表的免疫疗法,已为包括消化系统肿瘤[胃癌(GC)、结直肠癌(CRC)和肝细胞癌(HCC)]在内的多种肿瘤类型带来了持久的缓解和生存益处,尤其是那些有转移或复发病灶的患者。即便如此,并非所有胃肠道恶性肿瘤患者对抗程序性死亡蛋白1/程序性死亡配体1药物(抗PD-1/PD-L1)都有良好反应,这表明需要生物标志物来识别 responders和non-responders,以及预测临床结果。在预测基于免疫疗法的疗效时,PD-L1表达越来越成为一种潜在的生物标志物;但遗憾的是,仅靠PD-L1不足以区分患者。其他分子,如肿瘤突变负荷(TMB)、微卫星不稳定性(MSI)以及循环肿瘤DNA(ctDNA)等,也参与了进一步的探索。总体而言,由于存在固有局限性,目前消化系统肿瘤免疫疗法中仍没有完美或成熟的生物标志物,尤其是对于HCC。规范和统一现有生物标志物的评估,同时转向其他新型生物标志物可能是明智且可行的。