Estupiñán H Yesid, Berglöf Anna, Zain Rula, Smith C I Edvard
Department of Laboratory Medicine, Clinical Research Center, Karolinska Institutet, Karolinska University Hospital, Huddinge, Sweden.
Departamento de Ciencias Básicas, Universidad Industrial de Santander, Bucaramanga, Colombia.
Front Cell Dev Biol. 2021 Mar 11;9:630942. doi: 10.3389/fcell.2021.630942. eCollection 2021.
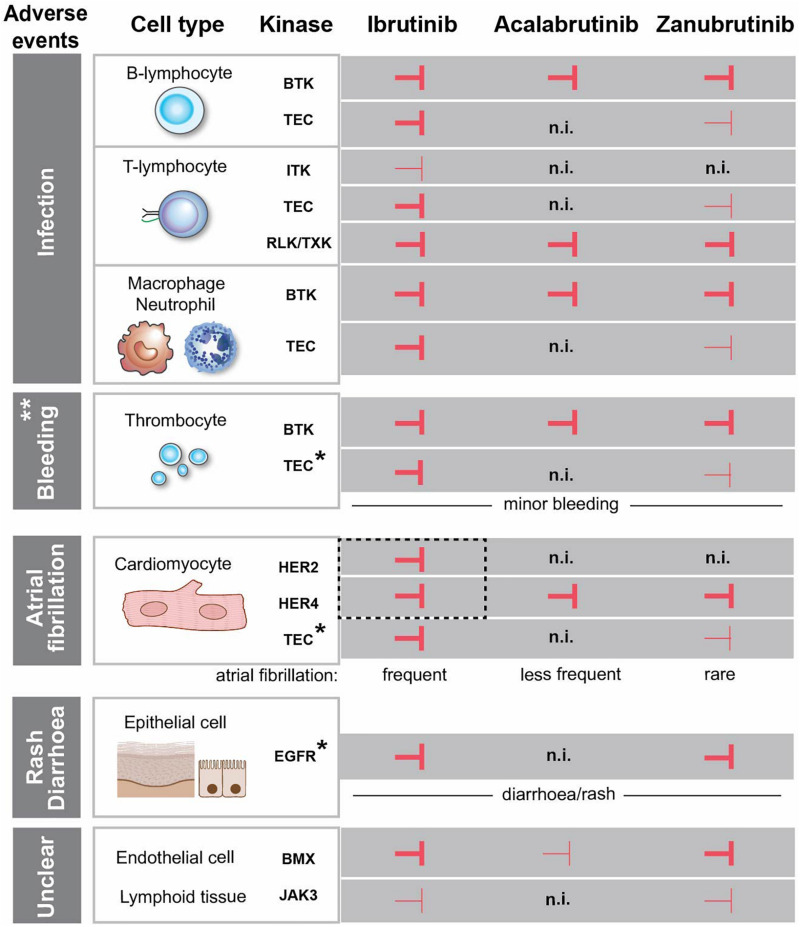
The cytoplasmic protein-tyrosine kinase BTK plays an essential role for differentiation and survival of B-lineage cells and, hence, represents a suitable drug target. The number of BTK inhibitors (BTKis) in the clinic has increased considerably and currently amounts to at least 22. First-in-class was ibrutinib, an irreversible binder forming a covalent bond to a cysteine in the catalytic region of the kinase, for which we have identified 228 active trials listed at ClinicalTrials.gov. Next-generation inhibitors, acalabrutinib and zanubrutinib, are approved both in the United States and in Europe, and zanubrutinib also in China, while tirabrutinib is currently only registered in Japan. In most cases, these compounds have been used for the treatment of B-lymphocyte tumors. However, an increasing number of trials instead addresses autoimmunity and inflammation in multiple sclerosis, rheumatoid arthritis, pemphigus and systemic lupus erythematosus with the use of either irreversibly binding inhibitors, e.g., evobrutinib and tolebrutinib, or reversibly binding inhibitors, like fenebrutinib. Adverse effects (AEs) have predominantly implicated inhibition of other kinases with a BTKi-binding cysteine in their catalytic domain. Analysis of the reported AEs suggests that ibrutinib-associated atrial fibrillation is caused by binding to ERBB2/HER2 and ERBB4/HER4. However, the binding pattern of BTKis to various additional kinases does not correlate with the common assumption that skin manifestations and diarrhoeas are off-target effects related to EGF receptor inhibition. Moreover, dermatological toxicities, diarrhoea, bleedings and invasive fungal infections often develop early after BTKi treatment initiation and subsequently subside. Conversely, cardiovascular AEs, like hypertension and various forms of heart disease, often persist.
细胞质蛋白酪氨酸激酶布鲁顿酪氨酸激酶(BTK)对B淋巴细胞的分化和存活起着至关重要的作用,因此是一个合适的药物靶点。临床中BTK抑制剂(BTKis)的数量已大幅增加,目前至少有22种。同类首创的是伊布替尼,它是一种不可逆结合剂,与激酶催化区域的一个半胱氨酸形成共价键,在ClinicalTrials.gov上我们已确定有228项关于它的正在进行的活性试验。新一代抑制剂阿卡替尼和泽布替尼在美国和欧洲均已获批,泽布替尼在中国也已获批,而替拉布替尼目前仅在日本注册。在大多数情况下,这些化合物已被用于治疗B淋巴细胞肿瘤。然而,越来越多的试验转而使用不可逆结合抑制剂(如依沃布替尼和托莱布替尼)或可逆结合抑制剂(如非奈布替尼)来治疗多发性硬化症、类风湿性关节炎、天疱疮和系统性红斑狼疮中的自身免疫和炎症。不良反应(AEs)主要与对其他激酶的抑制有关,这些激酶在其催化结构域中有一个与BTKi结合的半胱氨酸。对报告的不良反应的分析表明,伊布替尼相关的心房颤动是由与ERBB2/HER2和ERBB4/HER4结合引起的。然而,BTKis与各种其他激酶的结合模式与常见假设并不相关,该假设认为皮肤表现和腹泻是与表皮生长因子受体抑制相关的脱靶效应。此外,皮肤毒性、腹泻、出血和侵袭性真菌感染通常在开始BTKi治疗后早期出现,随后消退。相反,心血管不良反应,如高血压和各种形式的心脏病,往往会持续存在。