Li Shan-Shan, Niu Ming, Jing Jing, Huang Ying, Zhang Zi-Teng, Chen Shuai-Shuai, Shi Ge-Zi, He Xian, Zhang Hai-Zhu, Xiao Xiao-He, Zou Zheng-Sheng, Yu Yue-Cheng, Wang Jia-Bo
School of Pharmacy and Chemistry, Dali University, Dali, China.
Department of Liver Diseases, Fifth Medical Center of Chinese PLA General Hospital, Beijing, China.
Front Med (Lausanne). 2021 Mar 12;8:644376. doi: 10.3389/fmed.2021.644376. eCollection 2021.
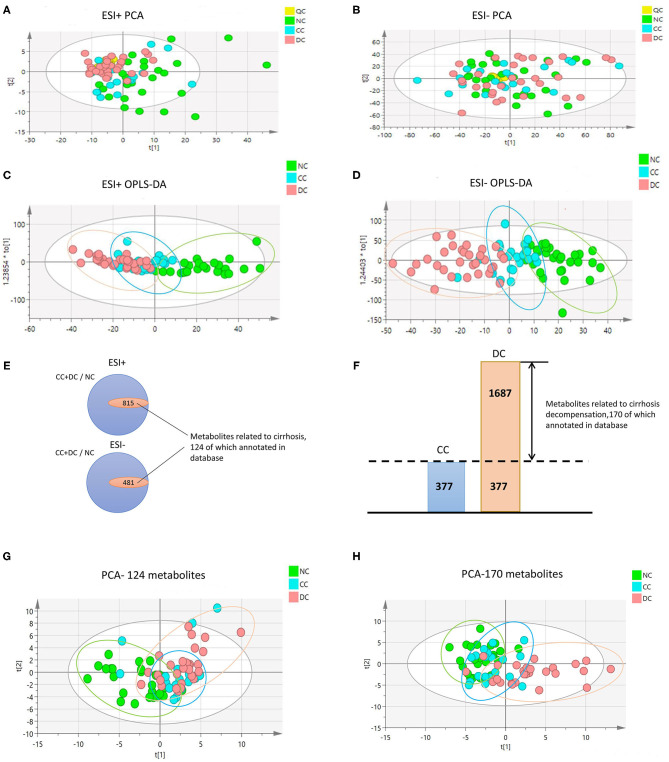
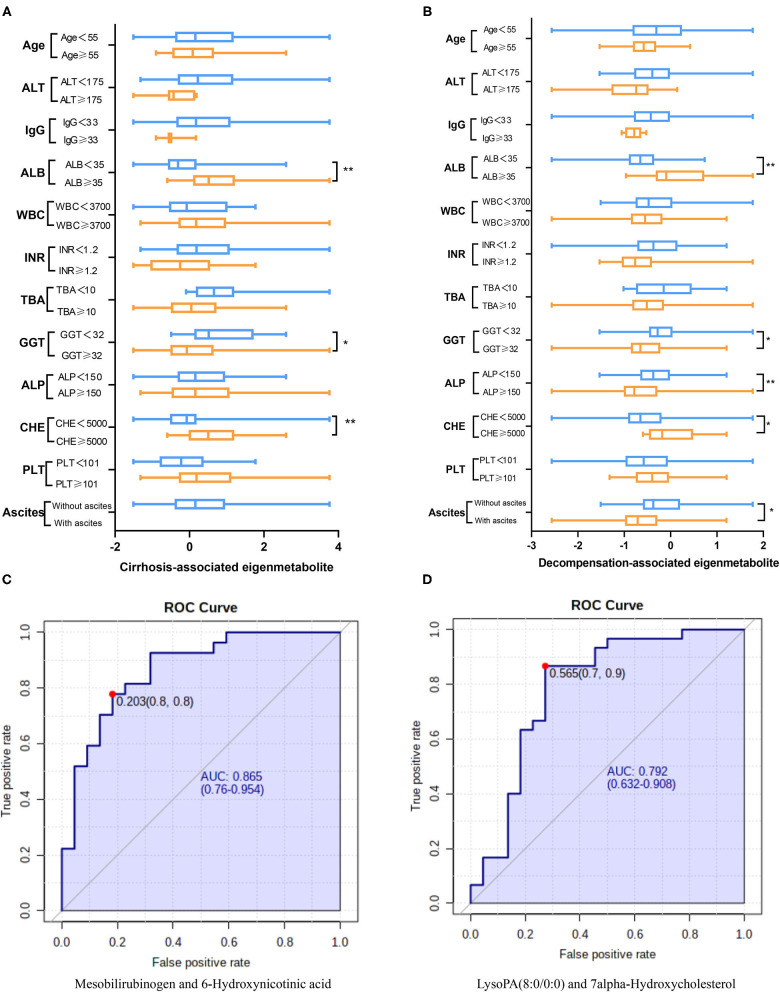
Autoimmune hepatitis (AIH) can progress into severe outcomes, i.e., decompensated cirrhosis, from remarkable and persistent inflammation in the liver. Considering the energy-expending nature of inflammation, we tried to define the metabolomics signatures of AIH to uncover the underlying mechanisms of cirrhosis development and its metabolic biomarkers. Untargeted metabolomics analysis was performed on sera samples from 79 AIH patients at the stages (phenotypes) of non-cirrhosis ( = 27), compensated cirrhosis ( = 22), and decompensated cirrhosis ( = 30). Pattern recognition was used to find unique metabolite fingerprints of cirrhosis with or without decompensation. Out of the 294 annotated metabolites identified, 2 metabolic fingerprints were found associated with the development of cirrhosis (independent of the decompensated state, 42 metabolites) and the evolution of decompensated cirrhosis (out of 47 metabolites), respectively. The cirrhosis-associated fingerprints (eigenmetabolite) showed better capability to differentiate cirrhosis from non-cirrhosis patients than the aminotransferase-to-platelet ratio index. From the metabolic fingerprints, we found two pairs of metabolites (Mesobilirubinogen/6-Hydroxynicotinic acid and LysoPA(8:0/0:0)/7alpha-Hydroxycholesterol) calculated as ratio of intensities, which revealed robust abilities to identify cirrhosis or predict decompensated patients, respectively. These phenotype-related fingerprint metabolites featured fundamental energy supply disturbance along with the development of AIH cirrhosis and progression to decompensation, which was characterized as increased lipolysis, enhanced proteolysis, and increased glycolysis. Remodeling of metabolism to meet the liver inflammation-related energy supply is one of the key signatures of AIH in the development of cirrhosis and decompensation. Therefore, drug regulation metabolism has great potential in the treatment of AIH.
自身免疫性肝炎(AIH)可因肝脏中显著且持续的炎症发展为严重后果,即失代偿性肝硬化。考虑到炎症消耗能量的特性,我们试图定义AIH的代谢组学特征,以揭示肝硬化发展的潜在机制及其代谢生物标志物。对79例处于非肝硬化(n = 27)、代偿性肝硬化(n = 22)和失代偿性肝硬化(n = 30)阶段(表型)的AIH患者的血清样本进行了非靶向代谢组学分析。采用模式识别方法寻找有无失代偿的肝硬化独特代谢物指纹图谱。在所鉴定出的294种注释代谢物中,分别发现2种代谢指纹图谱与肝硬化的发展(与失代偿状态无关,42种代谢物)和失代偿性肝硬化的进展(47种代谢物中的)相关。与肝硬化相关的指纹图谱(特征代谢物)在区分肝硬化患者和非肝硬化患者方面比转氨酶与血小板比值指数表现出更好的能力。从代谢指纹图谱中,我们发现两对以强度比值计算的代谢物(中胆红素原/6-羟基烟酸和溶血磷脂酸(8:0/0:0)/7α-羟基胆固醇),它们分别显示出识别肝硬化或预测失代偿患者的强大能力。这些与表型相关的指纹代谢物在AIH肝硬化发展及进展至失代偿过程中表现出基本能量供应紊乱,其特征为脂解增加、蛋白水解增强和糖酵解增加。代谢重塑以满足肝脏炎症相关的能量供应是AIH在肝硬化和失代偿发展过程中的关键特征之一。因此,药物调节代谢在AIH治疗中具有巨大潜力。