Lurie Antony, Amit Guy, Divakaramenon Syamkumar, Acosta J Gabriel, Healey Jeff S, Wong Jorge A
Faculty of Health Sciences, McMaster University, Hamilton, Ontario, Canada.
Department of Medicine, Hamilton Health Sciences Centre, Hamilton, Ontario, Canada.
CJC Open. 2020 Nov 13;3(3):303-310. doi: 10.1016/j.cjco.2020.11.002. eCollection 2021 Mar.
Intracardiac echocardiography and 3D mapping systems allow catheter ablation for atrial fibrillation (AF) to be conducted without fluoroscopy; however, the safety and effectiveness of fluoroless AF ablation are not well defined.
We examined consecutive radiofrequency AF catheter ablations at a large academic teaching hospital from November 2017 to July 2019. Outcomes for fluoroscopy-guided (N = 176) and fluoroless (N = 147) ablations were compared. Cases were designated as fluoroless at the outset of the procedure.
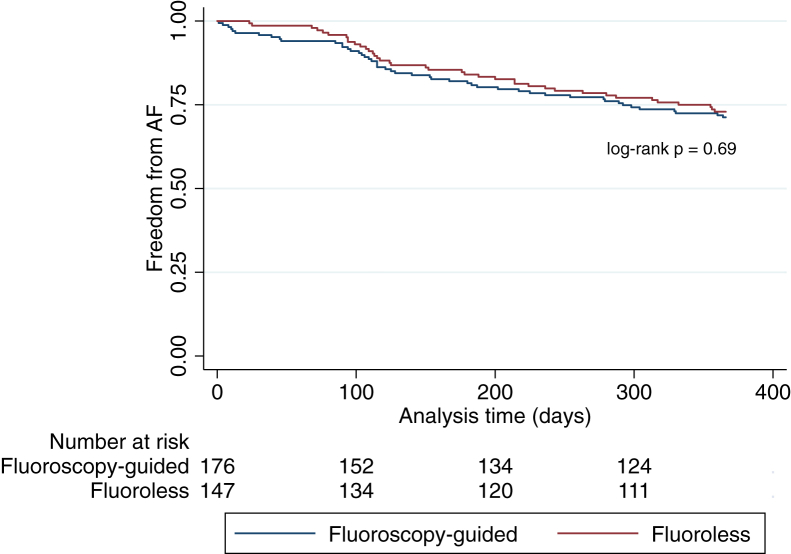
Mean age was 59.5 ± 10 years, 66.9% were male, 71.8% had paroxysmal AF, and the mean CHADS-VASc score was 1.7 ± 1.4. There were no differences in patient baseline characteristics. In the fluoroless group, minimal fluoroscopy was used in 17 patients (median, 3 seconds; interquartile range, 1.2-4.8). Mean procedure time, fluoroscopy time, and radiation dose (± standard deviation) were greater in the fluoroscopy group compared with the fluoroless group (194 ± 56 vs 176 ± 46 minutes, = 0.0021; 10.7 ± 6.6 vs 0.008 ± 0.03 minutes, < 0.0001; 2759.2 ± 1911 vs 5.4 ± 24 μGy m, < 0.0001). In multivariable linear regression models, fluoroless AF ablation was independently associated with reduced procedure times (ß = -16.5 minutes, = 0.01). Acute procedural success (95.5% vs 98.6%, = 0.1), complication rates (4.5% vs 2.0%, = 0.24), and 1-year AF recurrence rates (28.7% vs 27.1%, log-rank = 0.69) were similar between fluoroscopy and fluoroless groups. Excluding the 17 patients receiving fluoroscopy in the fluoroless group did not impact our results ( = 0.013). After exclusion of redo cases, fluoroless AF ablation was no longer associated with reduced procedure times (ß = -11.4 minutes, = 0.106).
Fluoroless radiofrequency AF ablation had similar effectiveness and safety compared with conventional fluoroscopy-guided AF ablation.
心内超声心动图和三维标测系统使房颤(AF)导管消融术可在无荧光透视的情况下进行;然而,无荧光房颤消融的安全性和有效性尚未明确界定。
我们对2017年11月至2019年7月在一家大型学术教学医院连续进行的射频房颤导管消融术进行了研究。比较了荧光透视引导下(N = 176)和无荧光(N = 147)消融的结果。手术一开始就将病例指定为无荧光。
平均年龄为59.5±10岁,男性占66.9%,71.8%患有阵发性房颤,平均CHADS-VASc评分为1.7±1.4。患者基线特征无差异。在无荧光组中,17例患者使用了最少的荧光透视(中位数,3秒;四分位间距,1.2 - 4.8)。与无荧光组相比,荧光透视组的平均手术时间、荧光透视时间和辐射剂量(±标准差)更长(194±56对176±46分钟,P = 0.0021;10.7±6.6对0.008±0.03分钟,P < 0.0001;2759.2±1911对5.4±24μGy m,P < 0.0001)。在多变量线性回归模型中,无荧光房颤消融与手术时间缩短独立相关(β = -16.5分钟,P = 0.01)。荧光透视组和无荧光组的急性手术成功率(95.5%对98.6%,P = 0.1)、并发症发生率(4.5%对2.0%,P = 0.24)和1年房颤复发率(28.7%对27.1%,对数秩检验P = 0.69)相似。排除无荧光组中接受荧光透视的17例患者不影响我们的结果(P = 0.013)。排除再次手术病例后,无荧光房颤消融与手术时间缩短不再相关(β = -11.4分钟,P = 0.106)。
与传统荧光透视引导下的房颤消融相比,无荧光射频房颤消融具有相似的有效性和安全性。