Fockele Callan Elswick, Duber Herbert C, Finegood Brad, Morse Sophie C, Whiteside Lauren K
Department of Emergency Medicine University of Washington Seattle Washington USA.
Department of Public Health Public Health-Seattle and King County Seattle Washington USA.
J Am Coll Emerg Physicians Open. 2021 Mar 23;2(2):e12408. doi: 10.1002/emp2.12408. eCollection 2021 Apr.
Opioid use disorder (OUD) is on the rise nationwide with increasing emergency department (ED) visits and deaths secondary to overdose. Although previous research has shown that patients who are started on buprenorphine in the ED have increased engagement in addiction treatment, access to on-demand medications for OUD is still limited, in part because of the need for linkages to outpatient care. The objective of this study is to describe emergency and outpatient providers' perception of local barriers to transitions of care for ED-initiated buprenorphine patients.
Purposive sampling was used to recruit key stakeholders, identified as physicians, addiction specialists, and hospital administrators, from 10 EDs and 11 outpatient clinics in King County, Washington. Twenty-one interviews were recorded and transcribed and then coded using an integrated deductive and inductive content analysis approach by 2 team members to verify accuracy of the analysis. Interview guides and coding were informed by the Consolidated Framework for Implementation Research (CFIR), which provides a structure of domains and constructs associated with effective implementation of evidence-based practice.
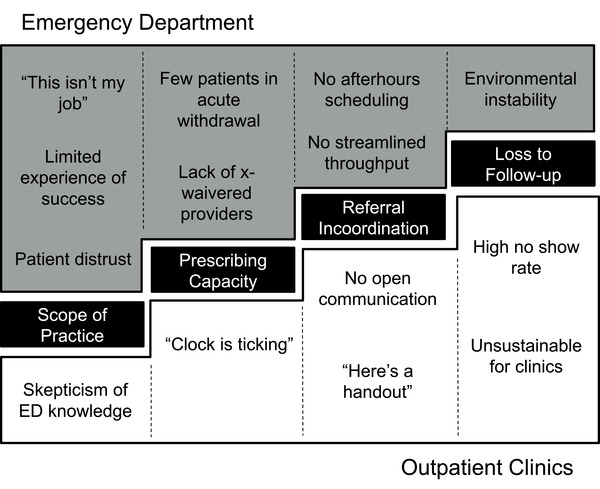
From the 21 interviews with emergency and outpatient providers, this study identified 4 barriers to transitions of care for ED-initiated buprenorphine patients: scope of practice, prescribing capacity, referral incoordination, and loss to follow-up.
Next steps for implementation of this intervention in a community setting include establishing a standard of care for treatment and referral for ED patients with OUD, increasing buprenorphine prescribing capacity, creating a central repository for streamlined referrals and follow-up, and supporting low-barrier scheduling and navigation services.
阿片类药物使用障碍(OUD)在全国范围内呈上升趋势,因过量用药导致的急诊科(ED)就诊和死亡人数不断增加。尽管先前的研究表明,在急诊科开始使用丁丙诺啡的患者对成瘾治疗的参与度有所提高,但获得按需治疗OUD的药物的机会仍然有限,部分原因是需要与门诊护理建立联系。本研究的目的是描述急诊和门诊医护人员对急诊科启动丁丙诺啡治疗的患者护理转接的当地障碍的看法。
采用目的抽样法,从华盛顿州金县的10个急诊科和11个门诊诊所招募关键利益相关者,确定为医生、成瘾专家和医院管理人员。记录并转录了21次访谈,然后由2名团队成员采用综合演绎和归纳内容分析方法进行编码,以验证分析的准确性。访谈指南和编码以实施研究综合框架(CFIR)为依据,该框架提供了与循证实践有效实施相关的领域和结构。
通过对21名急诊和门诊医护人员的访谈,本研究确定了急诊科启动丁丙诺啡治疗的患者护理转接的4个障碍:执业范围、处方能力、转诊不协调和失访。
在社区环境中实施该干预措施的下一步包括为患有OUD的急诊科患者建立治疗和转诊的护理标准,提高丁丙诺啡的处方能力,创建一个简化转诊和随访的中央资料库,并支持低门槛的排班和导航服务。