Division of Gastroenterology, Hepatology, and Endoscopy, Brigham and Women's Hospital, Harvard Medical School, Boston, MA.
Yale University School of Medicine, New Haven, CT.
J Clin Gastroenterol. 2022 Apr 1;56(4):324-330. doi: 10.1097/MCG.0000000000001526.
Although cannabis may worsen nausea and vomiting for patients with gastroparesis, it may also be an effective treatment for gastroparesis-related abdominal pain. Given conflicting data and a lack of current epidemiological evidence, we aimed to investigate the association of cannabis use on relevant clinical outcomes among hospitalized patients with gastroparesis.
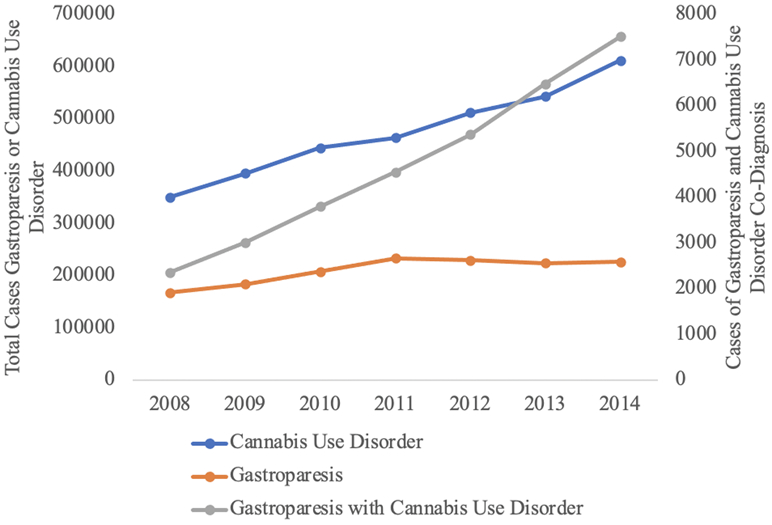
Patients with a diagnosis of gastroparesis were reviewed from the National Inpatient Sample (NIS) database between 2008 and 2014. Gastroparesis was identified by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes with patients classified based on a diagnosis of cannabis use disorder. Demographics, comorbidities, socioeconomic status, and outcomes were compared between cohorts using χ2 and analysis of variance. Logistic regression was then performed and annual trends also evaluated.
A total of 1,473,363 patients with gastroparesis were analyzed [n=33,085 (2.25%) of patients with concomitant cannabis use disorder]. Patients with gastroparesis and cannabis use disorder were more likely to be younger and male gender compared with nonusers (36.7±18.8 vs. 51.9±16.8; P<0.001 and 52.9% vs. 33.5%; P<0.001, respectively). Race/ethnicity was different between groups (P<0.001). Cannabis users had a lower median household income and were more likely to have Medicaid payor status (all P<0.001). Controlling for confounders, length of stay, and mortality were significantly decreased for patients with gastroparesis and cannabis use (all P<0.001).
While patients with gastroparesis and cannabis use disorder were younger, with a lower socioeconomic status, and disproportionately affected by psychiatric diagnoses, these patients had better hospitalization outcomes, including decreased length of stay and improved in-hospital mortality.
尽管大麻可能会使胃轻瘫患者的恶心和呕吐恶化,但它也可能是治疗胃轻瘫相关腹痛的有效方法。鉴于现有数据相互矛盾且缺乏当前的流行病学证据,我们旨在调查大麻使用与住院胃轻瘫患者相关临床结局的关联。
从 2008 年至 2014 年,我们从国家住院患者样本(NIS)数据库中对诊断为胃轻瘫的患者进行了回顾。通过国际疾病分类,第九修订版,临床修正(ICD-9-CM)代码诊断胃轻瘫,根据大麻使用障碍的诊断对患者进行分类。使用卡方检验和方差分析比较了队列之间的人口统计学,合并症,社会经济状况和结局。然后进行逻辑回归,并评估年度趋势。
共分析了 1473363 例胃轻瘫患者[共 33085 例(2.25%)患者同时患有大麻使用障碍]。与非使用者相比,患有胃轻瘫和大麻使用障碍的患者更年轻且更可能为男性(36.7±18.8 岁比 51.9±16.8 岁;P<0.001 和 52.9%比 33.5%;P<0.001)。组间种族/民族存在差异(P<0.001)。大麻使用者的中位数家庭收入较低,更可能拥有医疗补助保险支付人身份(均 P<0.001)。控制混杂因素后,患有胃轻瘫和大麻使用障碍的患者的住院时间和死亡率明显降低(均 P<0.001)。
尽管患有胃轻瘫和大麻使用障碍的患者年龄较小,社会经济地位较低,且受精神疾病诊断的影响不成比例,但这些患者的住院结局更好,包括住院时间缩短和住院死亡率提高。