Department of Cardiology, Cardiovascular Center, Beijing Friendship Hospital, Capital Medical University, Yongan Road 95, Xicheng District, 100050, Beijing, China.
Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Bei Li Shi Road 167, Xicheng District, 100037, Beijing, China.
BMC Cardiovasc Disord. 2021 Mar 30;21(1):157. doi: 10.1186/s12872-021-01962-2.
Acute hyperglycemia has been recognized as a robust predictor for occurrence of acute kidney injury (AKI) in nondiabetic patients with acute myocardial infarction (AMI), however, its discriminatory ability for AKI is unclear in diabetic patients after an AMI. Here, we investigated whether stress hyperglycemia ratio (SHR), a novel index with the combined evaluation of acute and chronic glycemic levels, may have a better predictive value of AKI as compared with admission glycemia alone in diabetic patients following AMI.
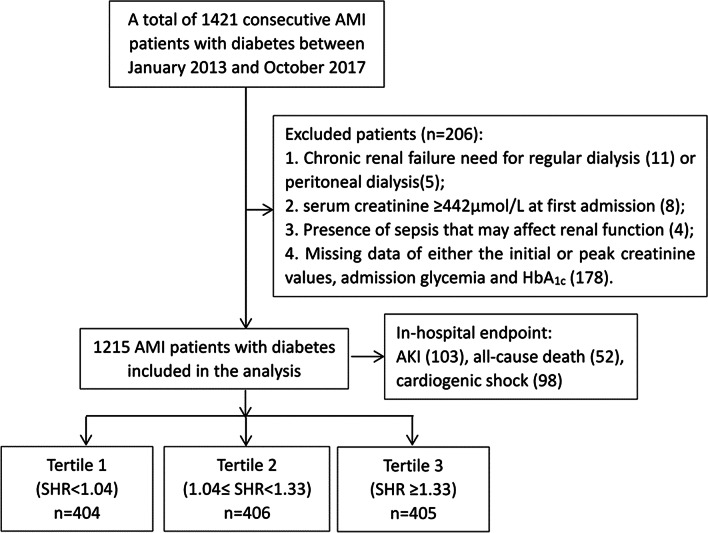
SHR was calculated with admission blood glucose (ABG) divided by the glycated hemoglobin-derived estimated average glucose. A total of 1215 diabetic patients with AMI were enrolled and divided according to SHR tertiles. Baseline characteristics and outcomes were compared. The primary endpoint was AKI and secondary endpoints included all-cause death and cardiogenic shock during hospitalization. The logistic regression analysis was performed to identify potential risk factors. Accuracy was defined with area under the curve (AUC) by a receiver-operating characteristic (ROC) curve analysis.
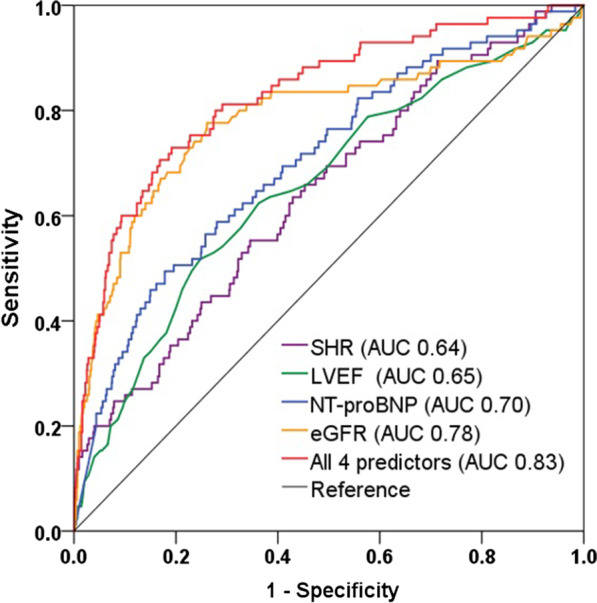
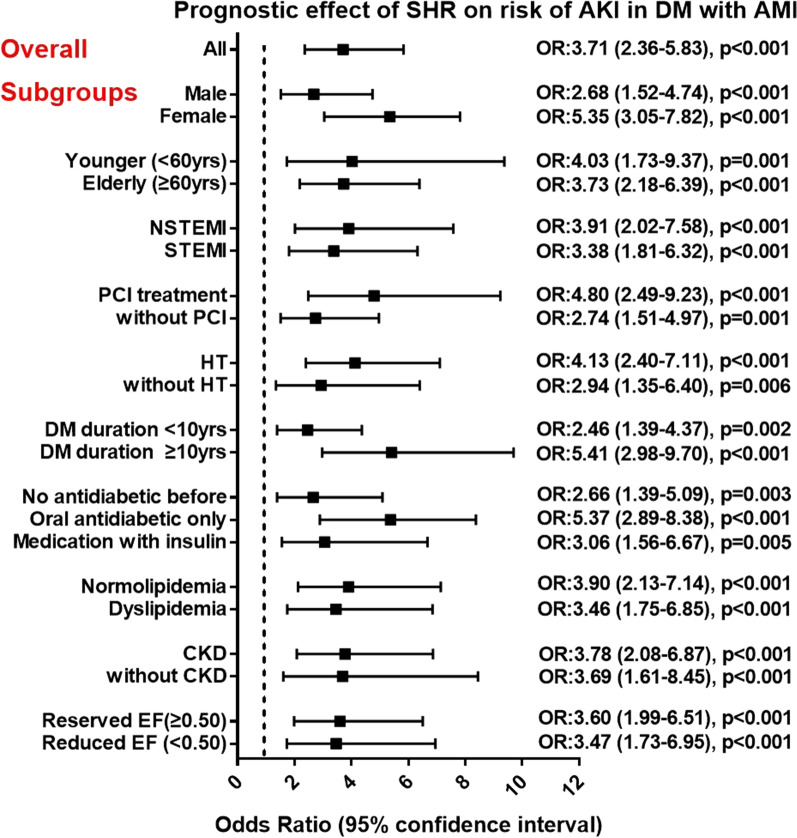
In AMI patients with diabetes, the incidence of AKI (4.4%, 7.8%, 13.0%; p < 0.001), all-cause death (2.7%, 3.6%, 6.4%; p = 0.027) and cardiogenic shock (4.9%, 7.6%, 11.6%; p = 0.002) all increased with the rising tertile levels of SHR. After multivariate adjustment, elevated SHR was significantly associated with an increased risk of AKI (odds ratio 3.18, 95% confidence interval: 1.99-5.09, p < 0.001) while ABG was no longer a risk factor of AKI. The SHR was also strongly related to the AKI risk in subgroups of patients. At ROC analysis, SHR accurately predicted AKI in overall (AUC 0.64) and a risk model consisted of SHR, left ventricular ejection fraction, N-terminal B-type natriuretic peptide, and estimated glomerular filtration rate (eGFR) yielded a superior predictive value (AUC 0.83) for AKI.
The novel index SHR is a better predictor of AKI and in-hospital mortality and morbidity than admission glycemia in AMI patients with diabetes.
急性高血糖已被认为是急性心肌梗死(AMI)非糖尿病患者发生急性肾损伤(AKI)的有力预测指标,但在 AMI 后糖尿病患者中,其对 AKI 的鉴别能力尚不清楚。在这里,我们研究了应激血糖比(SHR)作为一种新的指数,该指数综合评估了急性和慢性血糖水平,与 AMI 后糖尿病患者的入院血糖相比,是否对 AKI 具有更好的预测价值。
SHR 通过将入院时的血糖(ABG)除以糖化血红蛋白衍生的估计平均血糖计算得出。共纳入 1215 例 AMI 合并糖尿病患者,按 SHR 三分位数分组。比较基线特征和结局。主要终点是 AKI,次要终点包括住院期间全因死亡和心源性休克。采用 logistic 回归分析确定潜在的危险因素。通过受试者工作特征(ROC)曲线分析的曲线下面积(AUC)定义准确性。
在 AMI 合并糖尿病患者中,AKI 的发生率(4.4%、7.8%、13.0%;p<0.001)、全因死亡(2.7%、3.6%、6.4%;p=0.027)和心源性休克(4.9%、7.6%、11.6%;p=0.002)均随着 SHR 三分位水平的升高而升高。多变量调整后,升高的 SHR 与 AKI 风险增加显著相关(比值比 3.18,95%置信区间:1.99-5.09,p<0.001),而 ABG 不再是 AKI 的危险因素。SHR 与亚组患者的 AKI 风险也有很强的相关性。在 ROC 分析中,SHR 在整体(AUC 0.64)中准确预测 AKI,风险模型由 SHR、左心室射血分数、N 末端 B 型利钠肽和估算肾小球滤过率(eGFR)组成,对 AKI 的预测价值更高(AUC 0.83)。
在 AMI 合并糖尿病患者中,与入院血糖相比,新指数 SHR 是 AKI 和住院期间死亡率和发病率的更好预测指标。