Heart Center and Beijing Key Laboratory of Hypertension, Beijing Chaoyang Hospital, Capital Medical University, Beijing, China.
Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Ann Med. 2023 Dec;55(1):990-999. doi: 10.1080/07853890.2023.2186479.
The role of stress hyperglycemia in acute myocardial infarction (AMI) has long been emphasized. Recently, the stress hyperglycemia ratio (SHR), a novel index reflecting an acute glycemia rise, has shown a good predictive value in AMI. However, its prognostic power in myocardial infarction with nonobstructive coronary arteries (MINOCA) remains unclear.
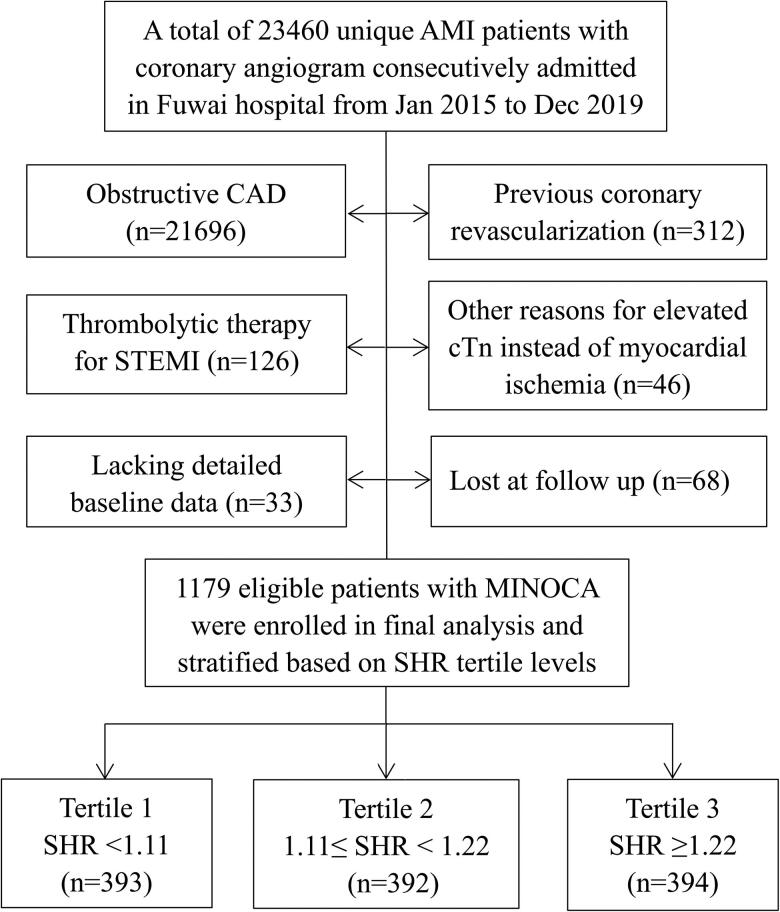
In a prospective cohort of 1179 patients with MINOCA, relationships between SHR levels and outcomes were analyzed. SHR was defined as acute-to-chronic glycemic ratio using admission blood glucose (ABG) and glycated hemoglobin. The primary endpoint was defined as major adverse cardiovascular events (MACE), including all-cause death, nonfatal MI, stroke, revascularization, and hospitalization for unstable angina or heart failure. Survival analyses and receiver-operating characteristic (ROC) curve analyses were performed.
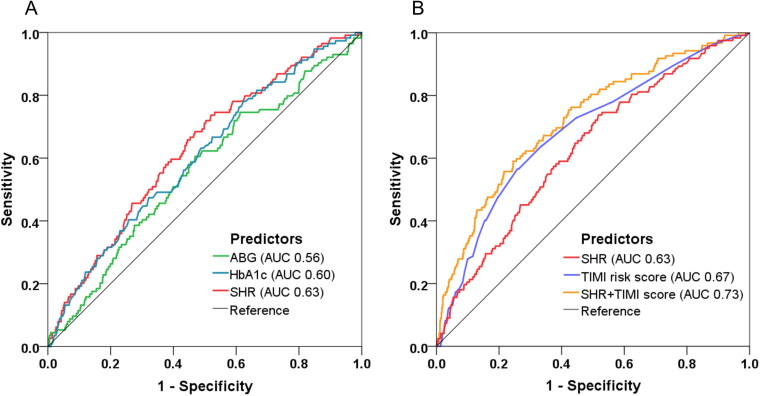
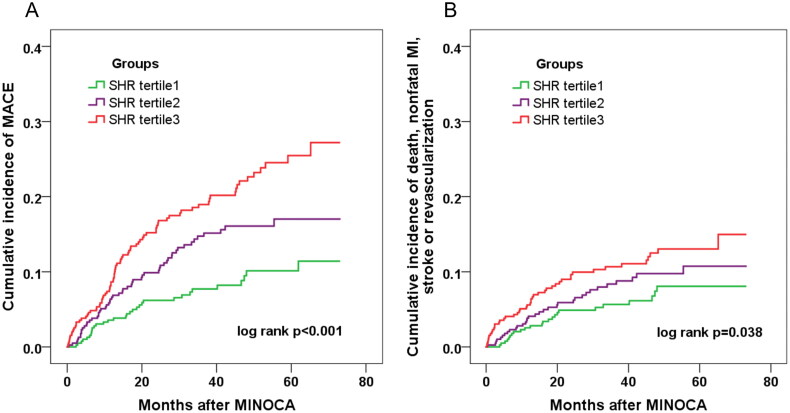
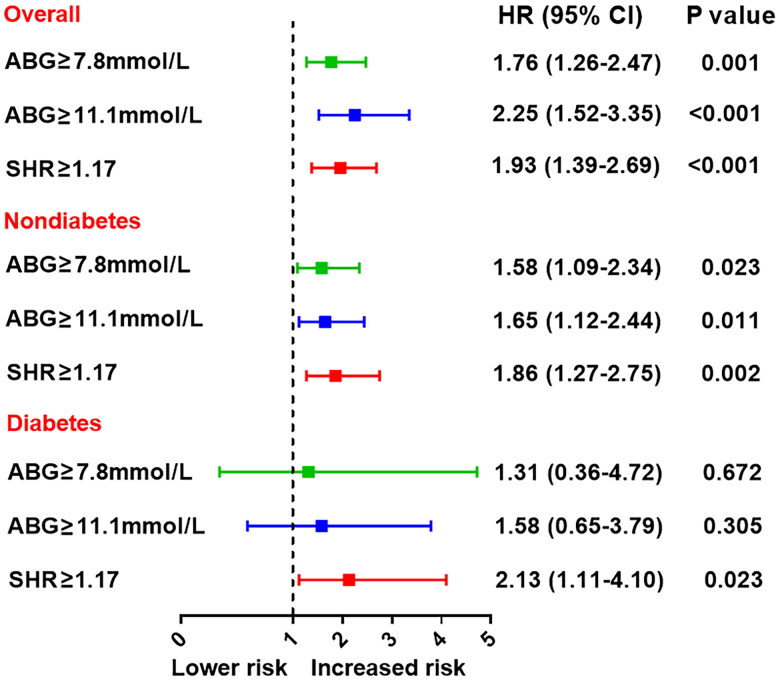
Over the median follow-up of 3.5 years, the incidence of MACE markedly increased with higher SHR tertile levels (8.1%, 14.0%, 20.5%; < 0.001). At multivariable Cox analysis, elevated SHR was independently associated with an increased risk of MACE (HR 2.30, 95% CI: 1.21-4.38, = 0.011). Patients with rising tertiles of SHR also had a significantly higher risk of MACE (tertile 1 as reference; tertile 2: HR 1.77, 95% CI: 1.14-2.73, = 0.010; tertile 3: HR 2.64, 95% CI: 1.75-3.98, < 0.001). SHR remained a robust predictor of MACE in patients with and without diabetes; whereas ABG was no longer associated with the MACE risk in diabetic patients. SHR showed an area under the curve of 0.63 for MACE prediction. By incorporating SHR to TIMI risk score, the combined model further improved the discrimination for MACE.
The SHR independently confers the cardiovascular risk after MINOCA, and may serve as a better predictor than glycemia at admission alone, particularly in those with diabetes.KEY MESSAGESStress hyperglycemia ratio (SHR) is independently associated with the prognosis in a distinct population with myocardial infarction with nonobstructive coronary arteries (MINOCA).SHR is a better predictor of prognosis than admission glycemia alone, especially in diabetic patients with MINOCA.SHR may serve as a prognostic marker for risk stratification as well as a potential target for tailored glucose-lowering treatment in MINOCA.
应激性高血糖在急性心肌梗死(AMI)中的作用一直受到重视。最近,反映急性血糖升高的新指标应激性高血糖比值(SHR)在 AMI 中显示出良好的预测价值。然而,其在非阻塞性冠状动脉心肌梗死(MINOCA)中的预后价值尚不清楚。
在一项前瞻性队列研究中,纳入了 1179 例 MINOCA 患者,分析了 SHR 水平与结局之间的关系。SHR 定义为入院时血糖(ABG)和糖化血红蛋白的急性到慢性血糖比值。主要终点定义为主要不良心血管事件(MACE),包括全因死亡、非致死性心肌梗死、卒中和血运重建以及不稳定型心绞痛或心力衰竭住院。进行生存分析和受试者工作特征(ROC)曲线分析。
在中位随访 3.5 年期间,随着 SHR 三分位水平的升高,MACE 的发生率明显增加(8.1%、14.0%、20.5%; < 0.001)。多变量 Cox 分析显示,升高的 SHR 与 MACE 风险增加独立相关(HR 2.30,95%CI:1.21-4.38, = 0.011)。SHR 三分位升高的患者发生 MACE 的风险也显著增加(以三分位 1 为参考;三分位 2:HR 1.77,95%CI:1.14-2.73, = 0.010;三分位 3:HR 2.64,95%CI:1.75-3.98, < 0.001)。SHR 仍然是有和无糖尿病患者 MACE 的有力预测因子;而 ABG 与糖尿病患者的 MACE 风险不再相关。SHR 对 MACE 的预测曲线下面积为 0.63。将 SHR 纳入到 TIMI 风险评分中,联合模型进一步提高了对 MACE 的鉴别能力。
SHR 独立于 MINOCA 后赋予心血管风险,并且可能比入院时的血糖单独更好地预测预后,尤其是在糖尿病患者中。