Deng Zhenfeng, Jin Zongrui, Qin Yonghui, Wei Mingqi, Wang Jilong, Lu Tingting, Zhang Ling, Zeng Jingjing, Bao Li, Guo Ya, Peng Minhao, Xu Banghao, Wen Zhang
Department of Hepatobiliary Surgery, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, China.
Department of Ultrasound, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, China.
World J Surg Oncol. 2021 Mar 30;19(1):95. doi: 10.1186/s12957-021-02199-1.
The feasibility of association liver partition and portal vein ligation for staged hepatectomy (ALPPS) for solitary huge hepatocellular carcinoma (HCC, maximal diameter ≥ 10 cm) remains uncertain. This study aims to evaluate the safety and the efficacy of ALPPS for patients with solitary huge HCC.
Twenty patients with solitary huge HCC who received ALPPS during January 2017 and December 2019 were retrospectively analyzed. The oncological characteristics of contemporaneous patients who underwent one-stage resection and transcatheter arterial chemoembolization (TACE) were compared using propensity score matching (PSM).
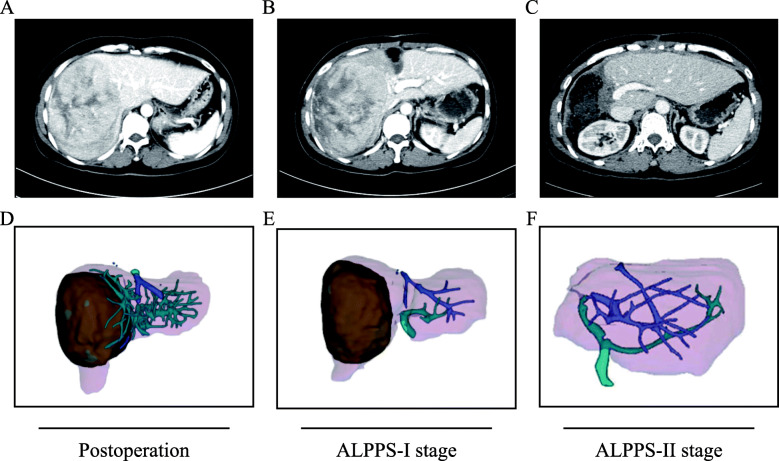
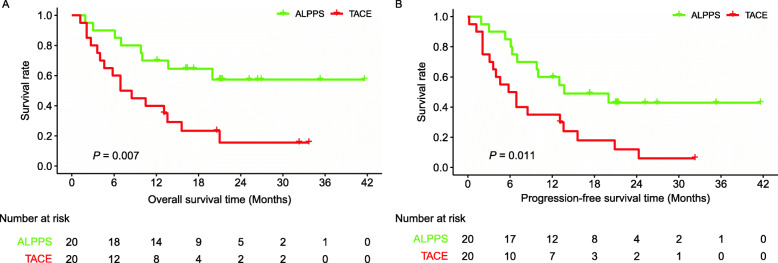
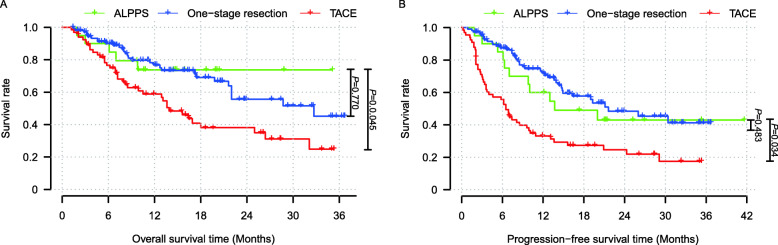
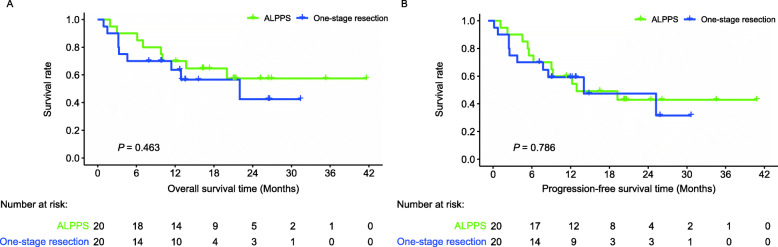
All patients underwent complete two-staged ALPPS. The median future liver remnant from the ALPPS-I stage to the ALPPS-II stage increased by 64.5% (range = 22.3-221.9%) with a median interval of 18 days (range = 10-54 days). The 90-day mortality rate after the ALPPS-II stage was 5%. The 1- and 3-year overall survival (OS) rates were 70.0% and 57.4%, respectively, whereas the 1- and 3-year progression-free survival (PFS) rates were 60.0% and 43.0%, respectively. In the one-to-one PSM analysis, the long-term survival of patients who received ALPPS was significantly better than those who received TACE (OS, P = 0.007; PFS, P = 0.011) but comparable with those who underwent one-stage resection (OS, P = 0.463; PFS, P = 0.786).
The surgical outcomes of ALPPS were superior to those of TACE and similar to those of one-stage resection. ALPPS is a safe and effective treatment strategy for patients with unresectable solitary huge HCC.
对于直径≥10cm的孤立性巨大肝细胞癌(HCC),联合肝脏分隔和门静脉结扎分期肝切除术(ALPPS)的可行性仍不确定。本研究旨在评估ALPPS治疗孤立性巨大HCC患者的安全性和疗效。
回顾性分析2017年1月至2019年12月期间接受ALPPS的20例孤立性巨大HCC患者。采用倾向评分匹配(PSM)比较同期接受一期肝切除和经动脉化疗栓塞术(TACE)患者的肿瘤学特征。
所有患者均成功完成两阶段ALPPS。从ALPPS-I期到ALPPS-II期,未来肝脏残余体积中位数增加了64.5%(范围=22.3-221.9%),中位间隔时间为18天(范围=10-54天)。ALPPS-II期术后90天死亡率为5%。1年和3年总生存率(OS)分别为70.0%和57.4%,而1年和3年无进展生存率(PFS)分别为60.0%和43.0%。在一对一PSM分析中,接受ALPPS患者的长期生存率显著优于接受TACE的患者(OS,P=0.007;PFS,P=0.011),但与接受一期肝切除的患者相当(OS,P=0.463;PFS,P=0.786)。
ALPPS的手术效果优于TACE,与一期肝切除相似。ALPPS是治疗不可切除的孤立性巨大HCC患者的一种安全有效的治疗策略。