School of Pharmacy, Sungkyunkwan University, Suwon, Korea.
VIAplus, Suwon, Korea.
Gut Liver. 2021 Nov 15;15(6):867-877. doi: 10.5009/gnl20353.
BACKGROUND/AIMS: Although anti-tumor necrosis factor (TNF) agents have been widely used to treat ulcerative colitis (UC), the real-world incidence of suboptimal response to anti-TNF agents has not been thoroughly investigated, especially among Asians.
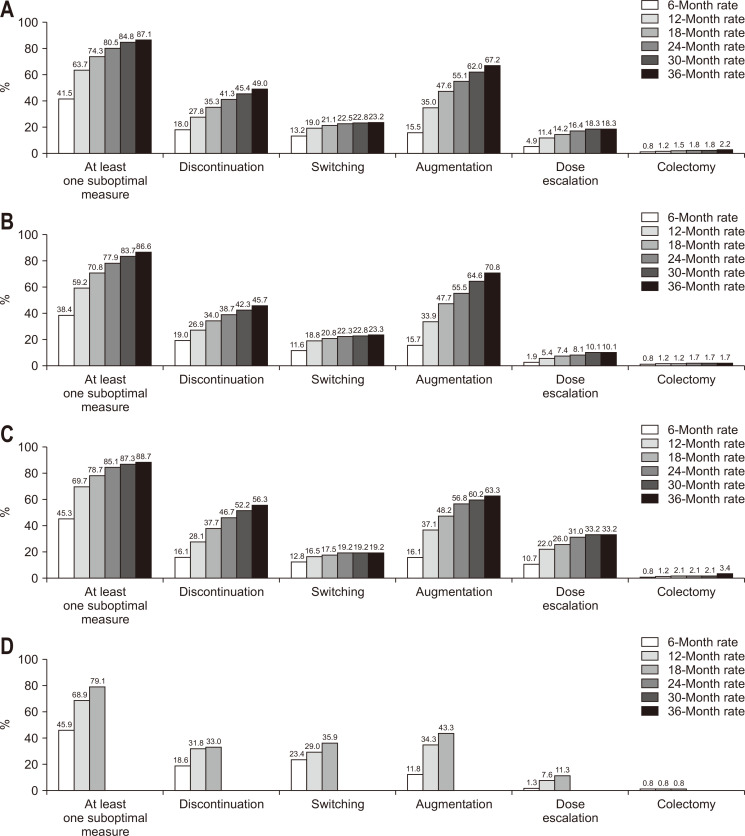
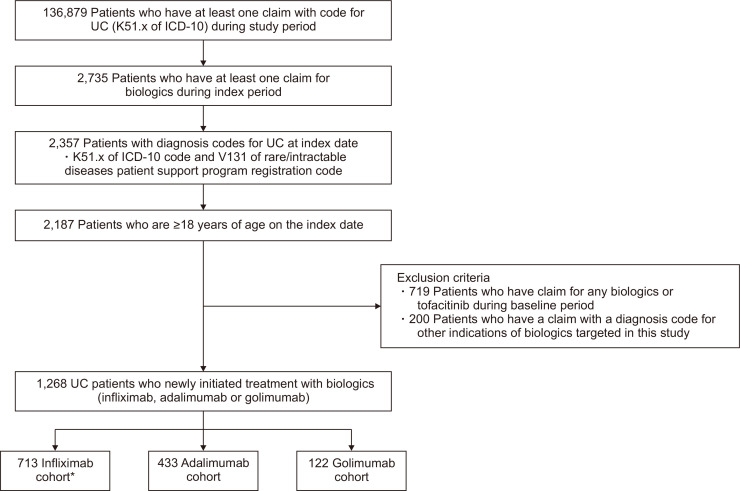
Using the Korean National Health Insurance database, we collected data on UC patients who initiated anti-TNF agents between July 1, 2014, and June 30, 2017. We assessed suboptimal responses, including anti-TNF discontinuation or dose escalation, switching to other biologics, augmentation with a non-biologic therapy, and the requirement for colectomy.
A total of 1,268 patients were included as new anti-TNF users (infliximab 713, adalimumab 433, golimumab 122). The proportion of patients who experienced at least one suboptimal response within 1 year among all patients was 63.5%, including 59.1%, 69.5%, and 68.0% of patients treated with infliximab, adalimumab, and golimumab, respectively. The cumulative incidences of at least one suboptimal response over time were 41.5%, 63.7%, 80.5%, and 87.1% at 6, 12, 24, and 36 months, respectively. Cox proportional hazards modeling revealed that adalimumab was associated with a higher risk of at least one suboptimal response (hazard ratio [HR], 1.29; 95% confidence interval [CI], 1.13 to 1.48), dose escalation (HR, 4.35; 95% CI, 2.97 to 6.38) and discontinuation (HR, 1.25; 95% CI, 1.03 to 1.52) than infliximab. Golimumab was associated with a higher risk of switching to other biologics than infliximab (HR, 1.78; 95% CI, 1.21 to 2.60).
More than half of Korean UC patients had suboptimal responses to anti-TNF agents within 1 year. UC patients treated with infliximab might be less prone to suboptimal responses than those treated with adalimumab or golimumab.
背景/目的:尽管抗肿瘤坏死因子(TNF)药物已被广泛用于治疗溃疡性结肠炎(UC),但对于抗 TNF 药物反应不佳的真实世界发生率,尤其是在亚洲人群中,尚未得到充分研究。
利用韩国国家健康保险数据库,我们收集了 2014 年 7 月 1 日至 2017 年 6 月 30 日期间开始使用抗 TNF 药物的 UC 患者的数据。我们评估了反应不佳的情况,包括抗 TNF 药物停药或剂量升级、改用其他生物制剂、联合非生物制剂治疗以及需要结肠切除术。
共有 1268 例患者被纳入新的抗 TNF 使用者(英夫利昔单抗 713 例,阿达木单抗 433 例,戈利木单抗 122 例)。所有患者中,在 1 年内至少出现 1 次反应不佳的患者比例为 63.5%,其中英夫利昔单抗、阿达木单抗和戈利木单抗治疗的患者分别为 59.1%、69.5%和 68.0%。随着时间的推移,至少出现 1 次反应不佳的累积发生率分别为 6 个月时 41.5%、12 个月时 63.7%、24 个月时 80.5%和 36 个月时 87.1%。Cox 比例风险模型显示,与英夫利昔单抗相比,阿达木单抗与至少 1 次反应不佳(风险比 [HR],1.29;95%置信区间 [CI],1.13 至 1.48)、剂量升级(HR,4.35;95%CI,2.97 至 6.38)和停药(HR,1.25;95%CI,1.03 至 1.52)的风险更高。与英夫利昔单抗相比,戈利木单抗与改用其他生物制剂的风险更高(HR,1.78;95%CI,1.21 至 2.60)。
超过一半的韩国 UC 患者在 1 年内对 TNF 拮抗剂药物的反应不佳。与英夫利昔单抗治疗的患者相比,接受阿达木单抗或戈利木单抗治疗的患者发生反应不佳的可能性可能较低。