Department of Neurosurgery.
Department of Ophthalmology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, People's Republic of China.
Medicine (Baltimore). 2021 Apr 2;100(13):e25346. doi: 10.1097/MD.0000000000025346.
Glioblastoma is the most lethal and common malignant brain tumor but rare in patients with neurofibromatosis type 1. The clinical findings and pathological findings with gene signatures in female patients have not been well clarified.
A 51-year-old female patient complained of headache and left limb weakness lasting for 20 days. The patient underwent a cesarean section 20 years ago and hysterectomy 1 year ago because of uterine leiomyomas. Multiple café-au-lait spots and neurofibromas were found over patient's chest, neck, back, and arms. The myodynamia of left distant and proximate epipodite were grade 0 and grade 1 respectively. The myodynamia of lower left limb was grade 3.
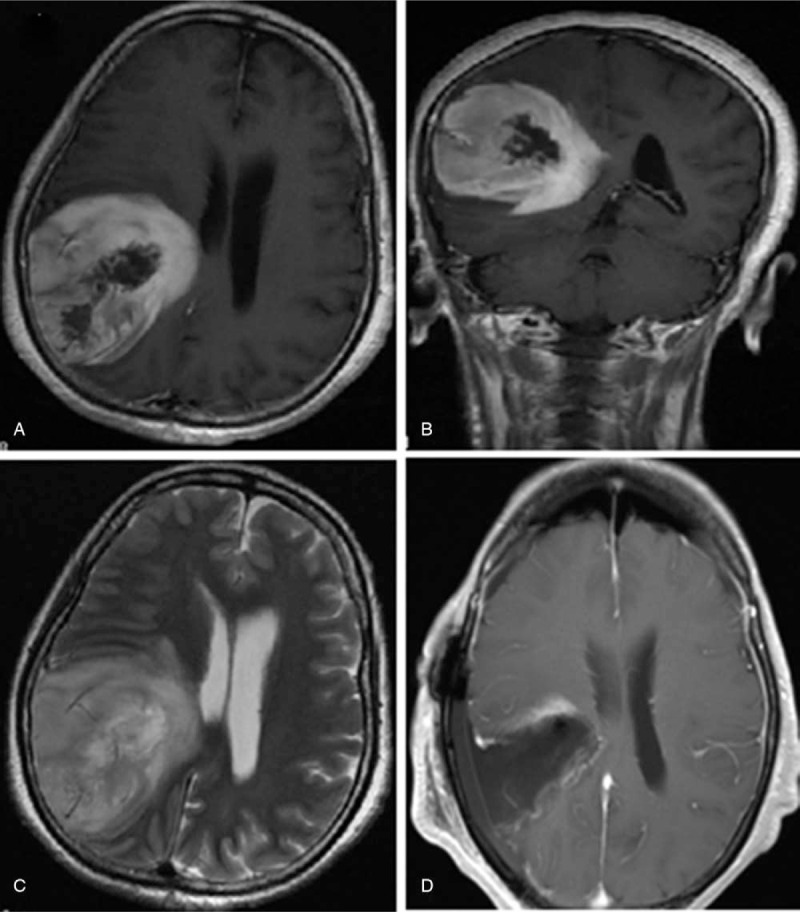
Magnetic resonance imaging revealed a malignant lesion which was most likely a glioblastoma in the right temporo-parietal lobe, approximately 5.6 × 5.9 × 6.9 cm in size with a rounded boundary.
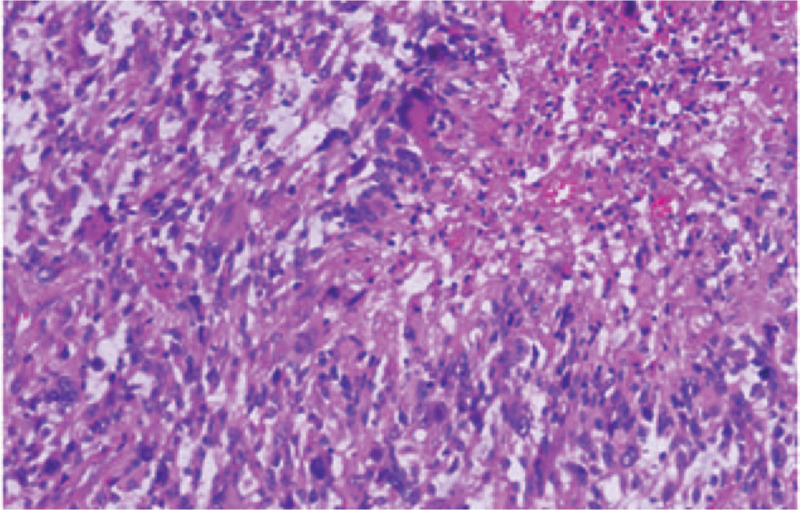
A right temporo-parietal craniotomy was performed to resect the space-occupying lesion for gross total removal. Then, the patient received concurrent chemoradiotherapy. Histological examination confirmed a glioblastoma without v-RAF murine sarcoma viral oncogene homolog B1 gene, isocitrate dehydrogenase 1 gene, and telomerase reverse transcriptase gene promoter mutations.
After surgery, the headache was relieved and the muscular strength of left limbs did improve. After receiving the standard treatment regimen, the patient was alive at 13 months follow-up.
This is the first reported glioblastoma in female neurofibromatosis type 1 patient without v-RAF murine sarcoma viral oncogene homolog B1 gene, isocitrate dehydrogenase 1 gene, and telomerase reverse transcriptase gene promoter mutations. Tumors in adult patients with these signatures were less aggressive with well-circumscribed border and had long-term survivals which strengthened the evidence that these patients may comprise a unique subset in glioblastoma.
胶质母细胞瘤是最致命和最常见的恶性脑肿瘤,但在神经纤维瘤病 1 型患者中很少见。女性患者的临床和病理表现以及基因特征尚未得到充分阐明。
一位 51 岁的女性患者因头痛和左侧肢体无力持续 20 天就诊。患者 20 年前因子宫肌瘤行剖宫产术,1 年前因子宫肌瘤行子宫切除术。患者胸部、颈部、背部和手臂多处出现咖啡牛奶斑和神经纤维瘤。左侧远侧和近侧附肢的肌力分别为 0 级和 1 级。左侧下肢肌力为 3 级。
磁共振成像显示右侧颞顶叶恶性病变,高度疑似为胶质母细胞瘤,大小约为 5.6×5.9×6.9cm,边界较圆。
行右侧颞顶部开颅术切除占位病变,达到大体全切除。然后,患者接受了同期放化疗。组织学检查证实为胶质母细胞瘤,无 v-RAF 鼠肉瘤病毒癌基因同源物 B1 基因、异柠檬酸脱氢酶 1 基因和端粒酶逆转录酶基因启动子突变。
手术后头痛缓解,左侧肢体肌力改善。接受标准治疗方案后,患者在 13 个月随访时仍存活。
这是首例报道的女性神经纤维瘤病 1 型伴 v-RAF 鼠肉瘤病毒癌基因同源物 B1 基因、异柠檬酸脱氢酶 1 基因和端粒酶逆转录酶基因启动子突变的胶质母细胞瘤患者。具有这些特征的成年患者的肿瘤侵袭性较低,边界较清晰,长期生存率较高,这进一步证明这些患者可能构成胶质母细胞瘤的一个独特亚群。