Division of Urology, Department of Surgery, University of Texas Medical Branch, Galveston.
Durham Veterans Affairs Health Care System, Durham, North Carolina.
JAMA Netw Open. 2021 Mar 1;4(3):e213800. doi: 10.1001/jamanetworkopen.2021.3800.
Management of high-risk non-muscle-invasive bladder cancer (NMIBC) represents a clinical challenge due to high failure rates despite prior bacillus Calmette-Guérin (BCG) therapy.
To describe real-world patient characteristics, long-term outcomes, and the economic burden in a population with high-risk NMIBC treated with BCG therapy.
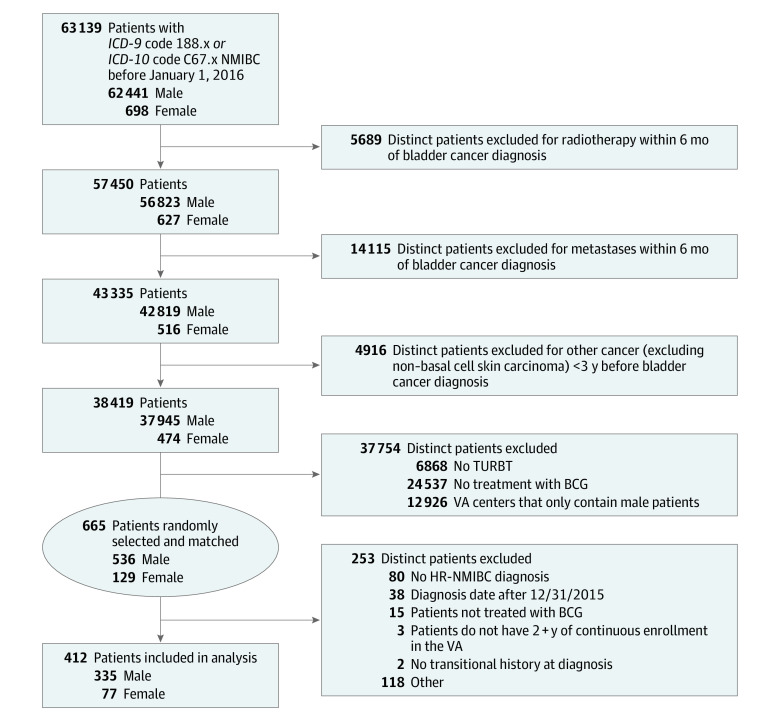
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study identified 412 patients with high-risk NMIBC from 63 139 patients diagnosed with bladder cancer who received at least 1 dose of BCG within Department of Veterans Affairs (VA) centers across the US from January 1, 2000, to December 31, 2015. Adequate induction BCG therapy was defined as at least 5 installations, and adequate maintenance BCG therapy was defined as at least 7 installations. Data were analyzed from January 2, 2020, to January 20, 2021.
Intravesical BCG therapy, including adequate induction BCG therapy, was defined as at least 5 intravesical instillations of BCG within 70 days from BCG therapy start date. Adequate maintenance BCG therapy was defined as at least 7 installations of BCG within 274 days of the start (the first instillation) of adequate induction BCG therapy (ie, adequate induction BCG plus some form of additional BCG).
The Kaplan-Meier method was used to estimate outcomes, including event-free survival. All-cause expenditures were summarized as medians with corresponding interquartile ranges (IQRs) and adjusted to 2019 USD.
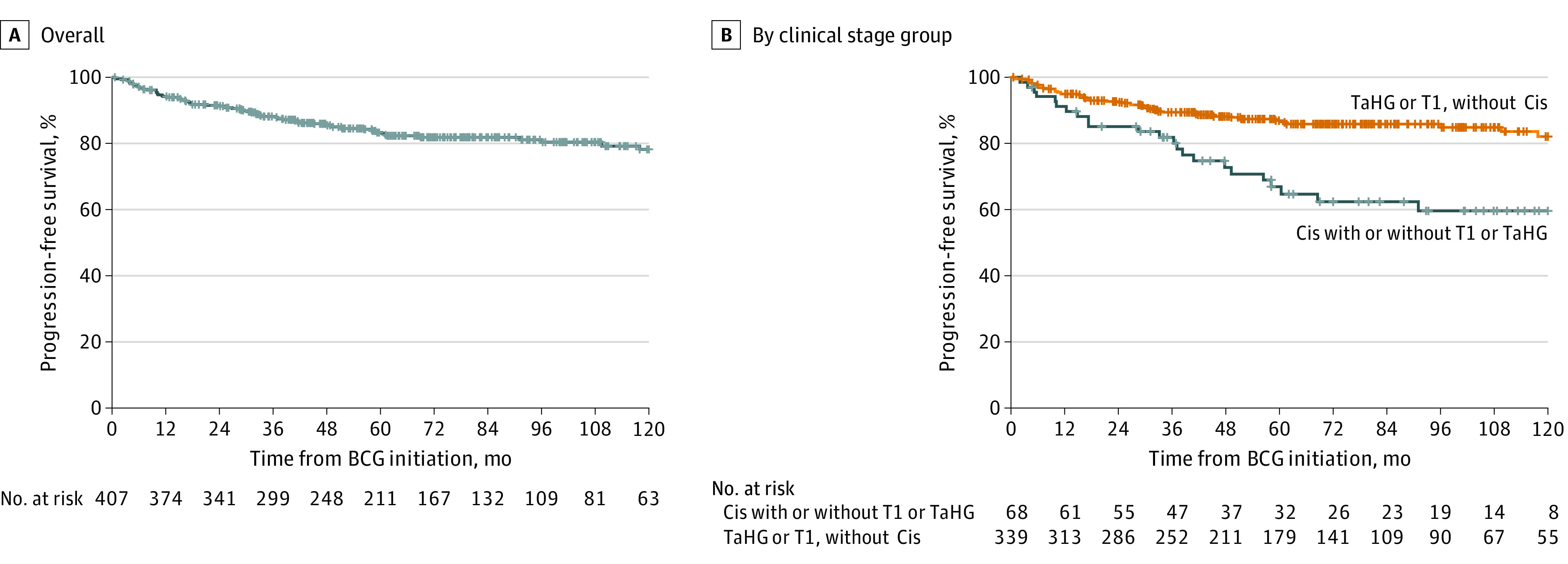
Of the 412 patients who met inclusion criteria, 335 (81%) were male and 77 (19%) were female, with a median age of 67 (IQR, 61-74) years. Follow-up was 2694 person-years. A total of 392 patients (95%) received adequate induction BCG therapy, and 152 (37%) received adequate BCG therapy. For all patients with high-risk NMIBC, the 10-year progression-free survival rate and disease-specific death rate were 78% and 92%, respectively. Patients with carcinoma in situ (Cis) had worse disease-free survival than those without Cis (hazard ratio [HR], 1.85; 95% CI, 1.34-2.56). Total median costs at 1 year were $29 459 (IQR, $14 991-$52 060); at 2 years, $55 267 (IQR, $28 667-$99 846); and at 5 years, $117 361 (IQR, $59 680-$211 298). Patients with progressive disease had significantly higher median 5-year costs ($232 729 [IQR, $151 321-$341 195] vs $94 879 [IQR, $52 498-$172 631]; P < .001), with outpatient care, pharmacy, and surgery-related costs contributing.
Despite adequate induction BCG therapy, only 37% of patients received adequate BCG therapy. Patients with Cis had increased risk of progression, and progression regardless of Cis was associated with significantly increased costs relative to patients without progression. Extrapolating cost figures, regardless of progression, resulted in nationwide costs at 1 year of $373 million for patients diagnosed with high-risk NMIBC in 2019.
尽管先前接受了卡介苗(BCG)治疗,但由于高复发率,高危非肌肉浸润性膀胱癌(NMIBC)的管理仍然是一个临床挑战。
描述高危 NMIBC 患者的真实特征、长期结局以及在接受 BCG 治疗的人群中的经济负担。
设计、地点和参与者:这项回顾性队列研究从美国退伍军人事务部(VA)中心诊断为膀胱癌并在 2000 年 1 月 1 日至 2015 年 12 月 31 日期间接受至少一剂 BCG 的 63139 名患者中确定了 412 名高危 NMIBC 患者。充分诱导 BCG 治疗定义为至少进行 5 次膀胱内灌注,充分维持 BCG 治疗定义为在充分诱导 BCG 治疗开始后(即开始 BCG 诱导治疗后的第 1 次)至少进行 7 次 BCG 灌注。数据于 2020 年 1 月 2 日至 2021 年 1 月 20 日进行分析。
膀胱内 BCG 治疗,包括充分诱导 BCG 治疗,定义为在 BCG 治疗开始后 70 天内至少进行 5 次膀胱内灌注。充分维持 BCG 治疗定义为在充分诱导 BCG 治疗开始后(即 BCG 诱导治疗加某种形式的额外 BCG)的 274 天内至少进行 7 次 BCG 灌注。
使用 Kaplan-Meier 方法估计结局,包括无事件生存。所有原因的支出均以中位数(四分位距)表示,并按 2019 年美元进行调整。
在符合纳入标准的 412 名患者中,335 名(81%)为男性,77 名(19%)为女性,中位年龄为 67 岁(四分位距,61-74 岁)。随访时间为 2694 人年。共有 392 名(95%)患者接受了充分的诱导 BCG 治疗,152 名(37%)患者接受了充分的 BCG 治疗。对于所有高危 NMIBC 患者,10 年无进展生存率和疾病特异性死亡率分别为 78%和 92%。患有原位癌(Cis)的患者无疾病生存率比没有 Cis 的患者差(风险比[HR],1.85;95%置信区间[CI],1.34-2.56)。1 年的总中位数费用为 29459 美元(四分位距,14991-52060 美元);2 年为 55267 美元(四分位距,28667-99846 美元);5 年为 117361 美元(四分位距,59680-211298 美元)。进展性疾病患者的 5 年中位数费用显著更高(232729 美元[四分位距,151321-341195 美元]与 94879 美元[四分位距,52498-172631 美元];P < .001),门诊护理、药房和手术相关费用也有所增加。
尽管进行了充分的诱导 BCG 治疗,但只有 37%的患者接受了充分的 BCG 治疗。患有 Cis 的患者发生进展的风险增加,无论是否发生 Cis,与未发生进展的患者相比,进展与显著增加的费用相关。无论进展情况如何,都要推断出费用数据,2019 年美国诊断出高危 NMIBC 的患者每年的全国费用为 3.73 亿美元。