Birmingham Women's Hospital, Birmingham, United Kingdom.
Directorate of Public Health and Wellbeing, Dudley Metropolitan Borough Council, Dudley, United Kingdom.
PLoS One. 2021 Mar 31;16(3):e0249233. doi: 10.1371/journal.pone.0249233. eCollection 2021.
To explore the effect of introducing 24/7 resident labour ward consultant presence on neonatal and maternal outcomes in a large obstetric unit in England.
Retrospective time sequence analysis of routinely collected data.
Obstetric unit of large teaching hospital in England.
Women and babies delivered between1 July 2011 and 30 June 2017. Births <24 weeks gestation or by planned caesarean section were excluded.
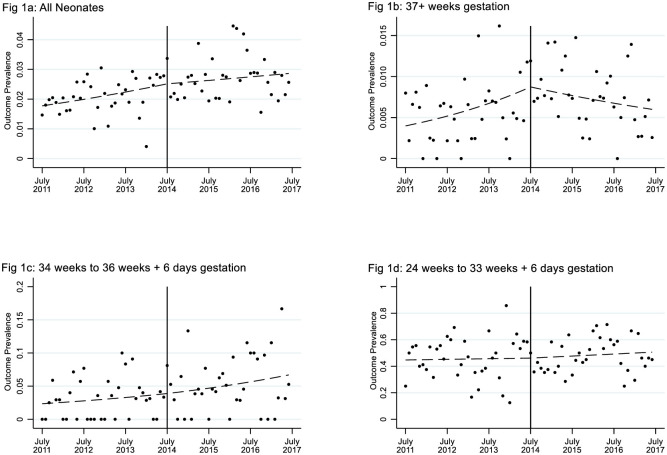
The primary composite outcome comprised intrapartum stillbirth, neonatal death, babies requiring therapeutic hypothermia, or admission to neonatal intensive care within three hours of birth. Secondary outcomes included markers of neonatal and maternal morbidity. Planned subgroup analyses investigated gestation (<34 weeks; 34-36 weeks; ≥37 weeks) and time of day.
17324 babies delivered before and 16110 after 24/7 consultant presence. The prevalence of the primary outcome increased by 0.65%, from 2.07% (359/17324) before 24/7 consultant presence to 2.72% (438/16110, P < 0.001) after 24/7 consultant presence which was consistent with an upward trend over time already well established before 24/7 consultant presence began (OR 1.09 p.a.; CI 1.04 to 1.13). Overall, there was no change in this trend associated with the transition to 24/7. However, in babies born ≥37 weeks gestation, the upward trend was reversed after implementation of 24/7 (OR 0.67 p.a.; CI 0.49 to 0.93; P = 0.017). No substantial differences were shown in other outcomes or subgroups.
Overall, resident consultant obstetrician presence 24/7 on labour ward was not associated with a change in a pre-existing trend of increasing adverse infant outcomes. However, 24/7 presence was associated with a reversal in increasing adverse outcomes for term babies.
探讨在英国一家大型产科单位引入 24/7 驻院妇产科顾问对新生儿和产妇结局的影响。
常规收集数据的回顾性时间序列分析。
英国一家大型教学医院的产科病房。
2011 年 7 月 1 日至 2017 年 6 月 30 日期间分娩的妇女和婴儿。排除 24 周以下或计划性剖宫产分娩的分娩。
主要复合结局包括产时死胎、新生儿死亡、需要治疗性低温治疗的婴儿或出生后 3 小时内入住新生儿重症监护病房。次要结局包括新生儿和产妇发病率的标志物。计划进行亚组分析,研究妊娠(<34 周;34-36 周;≥37 周)和一天中的时间。
在 24/7 顾问到场之前,有 17324 名婴儿分娩,在 24/7 顾问到场之后,有 16110 名婴儿分娩。主要结局的发生率增加了 0.65%,从 24/7 顾问到场前的 2.07%(359/17324)增加到 24/7 顾问到场后的 2.72%(438/16110,P<0.001),这与 24/7 顾问到场前已经确立的时间趋势一致(OR 1.09,每年;CI 1.04 至 1.13)。总体而言,向 24/7 过渡并没有改变这一趋势。然而,在≥37 周分娩的婴儿中,实施 24/7 后,上升趋势发生逆转(OR 0.67,每年;CI 0.49 至 0.93;P=0.017)。在其他结局或亚组中没有显示出实质性差异。
总体而言,驻院妇产科顾问 24/7 存在于产房与现有婴儿不良结局增加的趋势无关。然而,24/7 的存在与足月婴儿不良结局增加的趋势逆转有关。