Department of Cardiovascular Medicine, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Department of Clinical Epidemiology, Hyogo College of Medicine, Nishinomiya, Japan.
BMJ Open. 2021 Mar 31;11(3):e043683. doi: 10.1136/bmjopen-2020-043683.
To evaluate changes in demographics, clinical practices and long-term clinical outcomes of patients with ST segment-elevation myocardial infarction (STEMI) before and beyond 2010.
Multicentre retrospective cohort study.
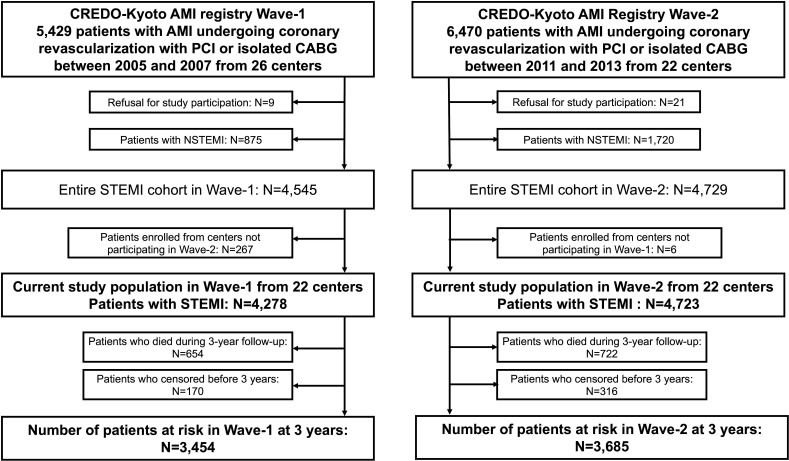
The Coronary Revascularization Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) AMI Registries Wave-1 (2005-2007, 26 centres) and Wave-2 (2011-2013, 22 centres).
9001 patients with STEMI who underwent coronary revascularisation (Wave-1: 4278 patients, Wave-2: 4723 patients).
The primary outcome was all-cause death at 3 years. The secondary outcomes were cardiovascular death, cardiac death, sudden cardiac death, non-cardiovascular death, non-cardiac death, myocardial infarction, definite stent thrombosis, stroke, hospitalisation for heart failure, major bleeding, target vessel revascularisation, ischaemia-driven target vessel revascularisation, any coronary revascularisation and any ischaemia-driven coronary revascularisation.
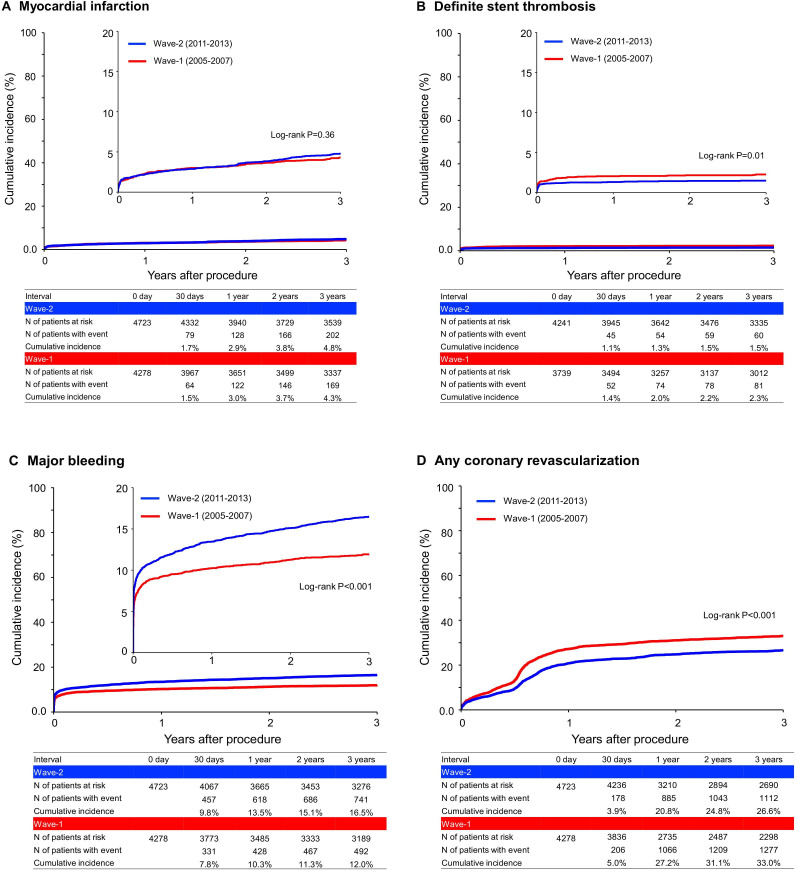
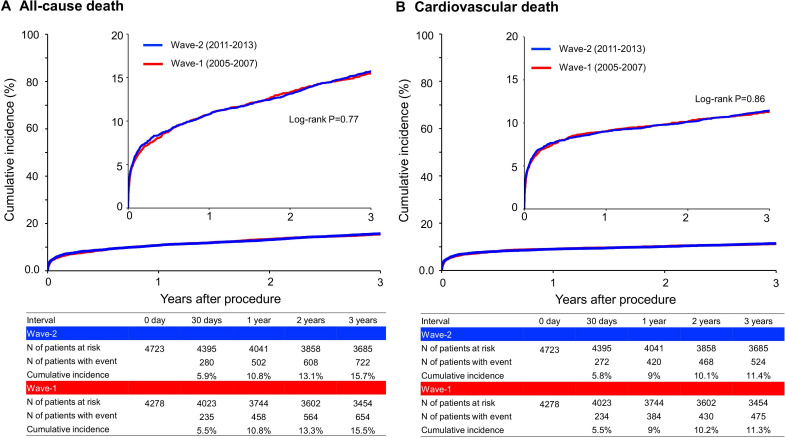
Patients in Wave-2 were older, more often had comorbidities and more often presented with cardiogenic shock than those in Wave-1. Patients in Wave-2 had shorter onset-to-balloon time and door-to-balloon time, were more frequently implanted drug-eluting stents, and received guideline-directed medication than those in Wave-1. The cumulative 3-year incidence of all-cause death was not significantly different between Wave-1 and Wave-2 (15.5% and 15.7%, p=0.77). The adjusted risk of all-cause death in Wave-2 relative to Wave-1 was not significant at 3 years (HR 0.92, 95% CI 0.83 to 1.03, p=0.14), but lower beyond 30 days (HR 0.86, 95% CI 0.75 to 0.98, p=0.03). The adjusted risks of Wave-2 relative to Wave-1 were significantly lower for definite stent thrombosis (HR 0.59, 95% CI 0.43 to 0.81, p=0.001) and for any coronary revascularisation (HR 0.75, 95% CI 0.69 to 0.81, p<0.001), but higher for major bleeding (HR 1.34, 95% CI 1.20 to 1.51, p=0.005).
We could not demonstrate improvement in 3-year mortality risk from Wave-1 to Wave-2, but we found reduction in mortality risk beyond 30 days. We also found risk reduction for definite stent thrombosis and any coronary revascularisation, but an increase in the risk of major bleeding from Wave-1 to Wave-2.
评估 2010 年前后 ST 段抬高型心肌梗死(STEMI)患者的人口统计学、临床实践和长期临床结局的变化。
多中心回顾性队列研究。
冠状动脉血运重建显示结果研究在京都(CREDO-京都)AMI 登记册波-1(2005-2007 年,26 个中心)和波-2(2011-2013 年,22 个中心)。
9001 例接受冠状动脉血运重建的 STEMI 患者(波-1:4278 例,波-2:4723 例)。
主要结局是 3 年全因死亡。次要结局是心血管死亡、心脏性死亡、心源性猝死、非心血管死亡、非心脏性死亡、心肌梗死、明确支架血栓形成、卒中和心力衰竭住院、大出血、靶血管血运重建、缺血驱动的靶血管血运重建、任何冠状动脉血运重建和任何缺血驱动的冠状动脉血运重建。
波-2 中的患者比波-1 中的患者年龄更大,合并症更多,更常出现心源性休克。波-2 中的患者发病至球囊时间和门球时间更短,更常植入药物洗脱支架,并接受指南指导的药物治疗。波-1 和波-2 患者的 3 年累积全因死亡率无显著差异(15.5%和 15.7%,p=0.77)。波-2 相对于波-1 的 3 年全因死亡风险调整后无显著差异(HR 0.92,95%CI 0.83 至 1.03,p=0.14),但在 30 天后降低(HR 0.86,95%CI 0.75 至 0.98,p=0.03)。波-2 相对于波-1 的风险调整后明确支架血栓形成(HR 0.59,95%CI 0.43 至 0.81,p=0.001)和任何冠状动脉血运重建(HR 0.75,95%CI 0.69 至 0.81,p<0.001)的风险显著降低,但大出血(HR 1.34,95%CI 1.20 至 1.51,p=0.005)的风险增加。
我们不能证明从波-1 到波-2 的 3 年死亡率风险有所改善,但我们发现 30 天后的死亡率风险有所降低。我们还发现明确支架血栓形成和任何冠状动脉血运重建的风险降低,但波-1 到波-2 的大出血风险增加。