Department of Cardiovascular Medicine, Chiba University Graduate School of Medicine.
Department of Cardiovascular Medicine, Eastern Chiba Medical Center.
J Atheroscler Thromb. 2023 Mar 1;30(3):299-309. doi: 10.5551/jat.63576. Epub 2022 May 25.
The Academic Research Consortium (ARC) has proposed international criteria to standardize the definition of high bleeding risk (HBR) in patients undergoing percutaneous coronary intervention (PCI). In this context, Japan has also established its own guidelines, that is, the Japanese version of HBR (J-HBR) criteria. However, the J-HBR criteria have not been fully validated, especially in patients with acute myocardial infarction (MI).
This bi-center registry included 1079 patients with acute MI undergoing primary PCI in a contemporary setting. Patient bleeding risks were evaluated using the ARC-HBR and J-HBR criteria. The primary endpoint was rates of major bleeding events (Bleeding Academic Research Consortium type 3 or 5) at 1 year.
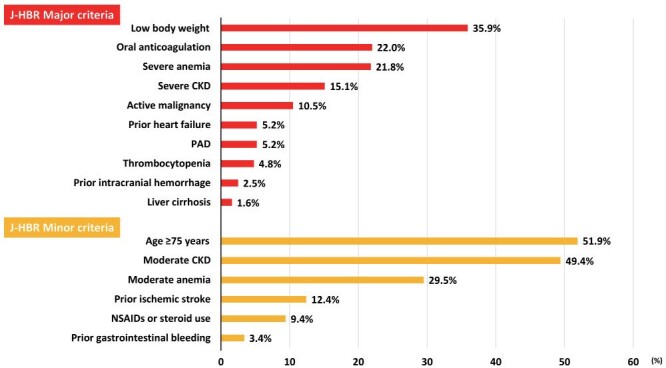
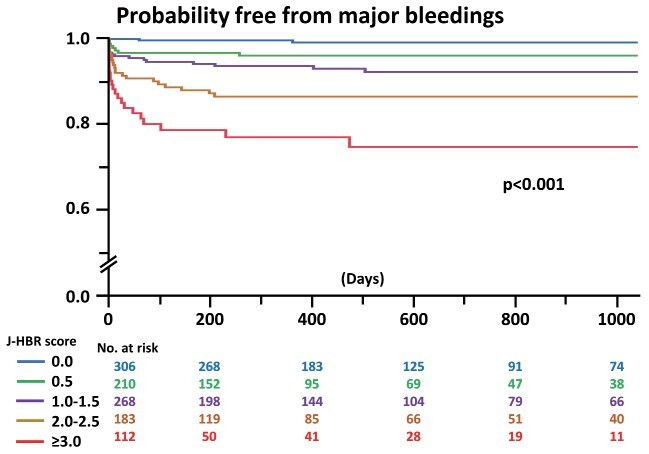
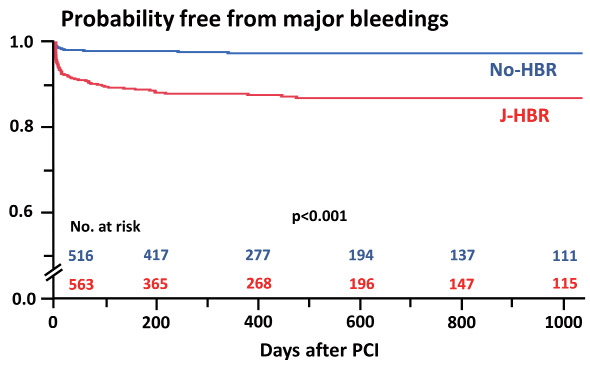
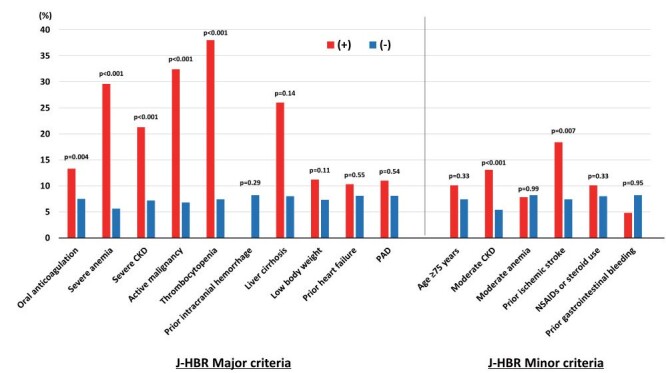
Of the 1079 patients, 505 (46.8%) and 563 (52.2%) met the ARC-HBR and J-HBR criteria, respectively. Patients who met the J-HBR criteria were found to have a higher rate of major bleeding events at 1 year than those who did not (12.8% vs. 3.3%, p<0.001). When patients were scored and stratified using the J-HBR major and minor criteria, risks of major bleedings were progressively increased with the increase in the number of J-HBR criteria. In the receiver operating characteristic curve analysis, the ARC-HBR and J-HBR significantly predicted subsequent major bleedings after PCI, with ARC-HBR having greater predictive ability than J-HBR.
More than half of the patients with acute MI undergoing primary PCI in Japan met the J-HBR criteria. Although the J-HBR criteria successfully identified patients who were likely to develop major bleeding events after primary PCI, the superiority of J-HBR to ARC-HBR in predicting bleeding outcomes warrants further investigation.
学术研究联合会(ARC)提出了国际标准,以规范接受经皮冠状动脉介入治疗(PCI)的患者中高出血风险(HBR)的定义。在此背景下,日本也制定了自己的指南,即日本版 HBR(J-HBR)标准。然而,J-HBR 标准尚未得到充分验证,尤其是在急性心肌梗死(MI)患者中。
本双中心注册研究纳入了 1079 例在当代背景下接受直接 PCI 的急性 MI 患者。使用 ARC-HBR 和 J-HBR 标准评估患者出血风险。主要终点是 1 年时主要出血事件(BARC 3 型或 5 型)发生率。
在 1079 例患者中,分别有 505 例(46.8%)和 563 例(52.2%)符合 ARC-HBR 和 J-HBR 标准。符合 J-HBR 标准的患者在 1 年时发生主要出血事件的发生率高于不符合的患者(12.8% vs. 3.3%,p<0.001)。当根据 J-HBR 主要和次要标准对患者进行评分和分层时,随着 J-HBR 标准数量的增加,发生大出血的风险逐渐增加。在接受者操作特征曲线分析中,ARC-HBR 和 J-HBR 均能显著预测 PCI 后主要出血事件,ARC-HBR 的预测能力大于 J-HBR。
日本接受直接 PCI 的急性 MI 患者中,有一半以上符合 J-HBR 标准。虽然 J-HBR 标准成功识别了接受直接 PCI 后发生大出血事件的高风险患者,但 J-HBR 在预测出血结局方面优于 ARC-HBR,尚需进一步研究。