Zeng Lichuan, Liao Huaqiang, Ren Fengchun, Zhang Yudong, Wang Qu, Xie Mingguo
Department of Radiology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, People's Republic of China.
Department of Ultrasound, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, People's Republic of China.
Int J Gen Med. 2021 Mar 23;14:1013-1022. doi: 10.2147/IJGM.S302434. eCollection 2021.
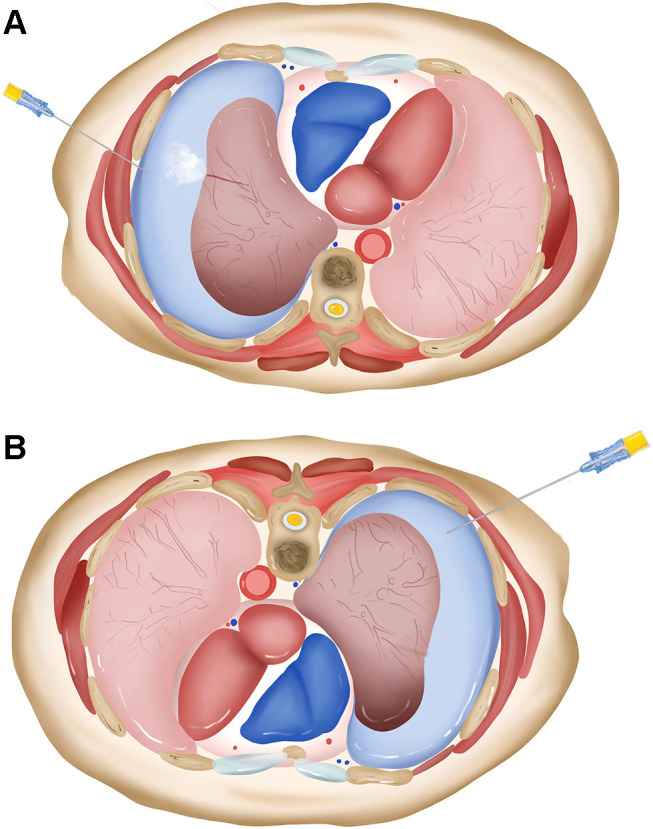
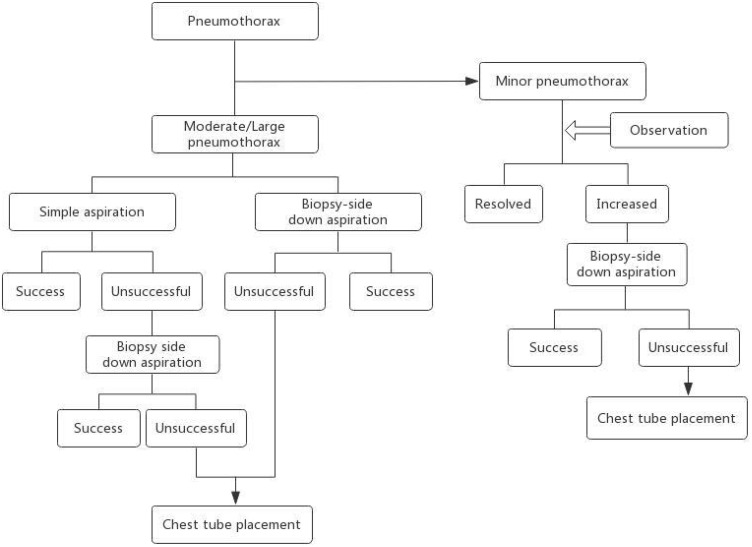
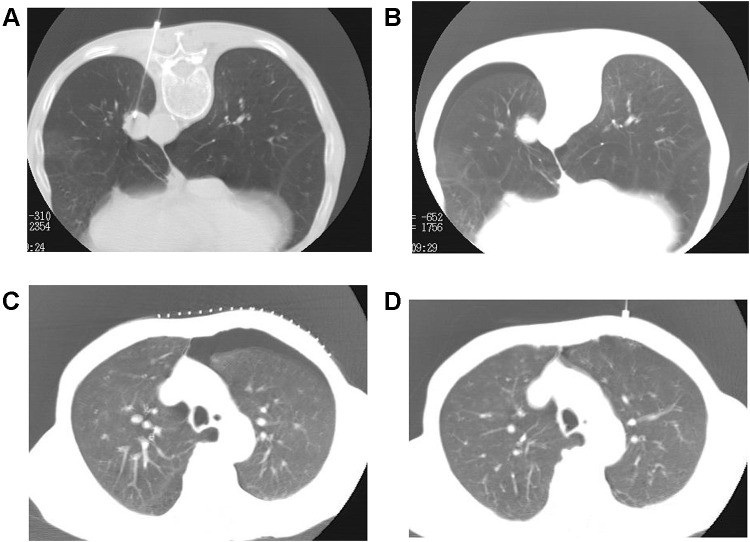
Percutaneous computed tomography (CT)-guided transthoracic needle biopsy (TTNB) is a valuable procedure for obtaining tissue or cells for diagnosis, which is especially indispensable in thoracic oncology. Pneumothorax and hemoptysis are the most common complications of percutaneous needle biopsy of the lung. According to reports published over the past decades, pneumothorax incidence in patients who underwent TTNB greatly varies. The morbidity of pneumothorax after CT-guided TTNB depends on several factors, including size and depth of lesions, emphysema, the number of pleural surfaces and fissure crossed, etc. Attention to biopsy planning and technique and post-biopsy precautions help to prevent or minimize potential complications. Many measures can be taken to help prevent the progression of a pneumothorax, which in turn might reduce the number of pneumothoraces requiring chest tube placement. A multitude of therapeutic options is available for the treatment of pneumothorax, varying from observation and oxygen treatment, simple manual aspiration, to chest tube placement. When a pneumothorax develops during the biopsy procedure, it can be manually aspirated after the needle is retracted back into the pleural space or by inserting a separate needle into the pleural space. Biopsy side down positioning of the patient after biopsy significantly reduces the incidence of pneumothorax and the requirement of chest tube placement. Aspiration in biopsy side down position is also recommended for treating pneumothorax when simple manual aspiration is unsuccessful or delayed pneumothorax occurred. Chest tube placement is an important treatment strategy for patients with a large or symptomatic pneumothorax. Clinicians are encouraged to understand the development, prevention, and treatment of pneumothorax. Efforts should be made to reduce the incidence of pneumothorax in biopsy planning and post-biopsy precautions. When pneumothorax occurs, appropriate treatment should be adopted to reduce the risk of worsening pneumothorax.
经皮计算机断层扫描(CT)引导下的经胸壁针吸活检(TTNB)是获取组织或细胞用于诊断的一项重要检查,在胸部肿瘤学中尤为不可或缺。气胸和咯血是经皮肺穿刺活检最常见的并发症。根据过去几十年发表的报告,接受TTNB的患者气胸发生率差异很大。CT引导下TTNB术后气胸的发生率取决于多个因素,包括病变的大小和深度、肺气肿、穿过的胸膜表面和肺裂的数量等。重视活检规划、技术以及活检后的预防措施有助于预防或减少潜在并发症。可以采取多种措施来帮助预防气胸进展,进而可能减少需要放置胸腔引流管的气胸数量。对于气胸的治疗有多种选择,从观察和吸氧治疗、单纯手动抽气到放置胸腔引流管。在活检过程中发生气胸时,可在针退回到胸膜腔后手动抽气,或通过插入一根单独的针进入胸膜腔进行抽气。活检后患者采取活检侧朝下的体位可显著降低气胸发生率和胸腔引流管放置的需求。当单纯手动抽气不成功或发生延迟性气胸时,也建议在活检侧朝下的体位下进行抽气治疗气胸。对于大量气胸或有症状的气胸患者,放置胸腔引流管是一项重要的治疗策略。鼓励临床医生了解气胸的发生、预防和治疗。应在活检规划和活检后预防措施中努力降低气胸发生率。气胸发生时,应采取适当治疗以降低气胸恶化的风险。