Department of Anesthesia and Pain Management; University Health Network, Sinai Health System, Women's College Hospital, University of Toronto, Toronto, Ontario, Canada.
Peter Munk Cardiac Centre and Toronto General Hospital Research Institute, University Health Network, Toronto, Ontario, Canada.
JAMA Netw Open. 2021 Apr 1;4(4):e213936. doi: 10.1001/jamanetworkopen.2021.3936.
Approximately 15% of patients undergoing cardiac surgery receive frozen plasma (FP) for bleeding. Four-factor prothrombin complex concentrates (PCCs) have logistical and safety advantages over FP and may be a suitable alternative.
To determine the proportion of patients who received PCC and then required FP, explore hemostatic effects and safety, and assess the feasibility of study procedures.
DESIGN, SETTING, AND PARTICIPANTS: Parallel-group randomized pilot study conducted at 2 Canadian hospitals. Adult patients requiring coagulation factor replacement for bleeding during cardiac surgery (from September 23, 2019, to June 19, 2020; final 28-day follow-up visit, July 17, 2020). Data analysis was initiated on September 15, 2020.
Prothrombin complex concentrate (1500 IU for patients weighing ≤60 kg and 2000 IU for patients weighing >60 kg) or FP (3 U for patients weighing ≤60 kg and 4 U for patients weighing >60 kg), repeated once as needed within 24 hours (FP used for any subsequent doses in both groups). Patients and outcome assessors were blinded to treatment allocation.
Hemostatic effectiveness (whether patients received any hemostatic therapies from 60 minutes to 4 and 24 hours after initiation of the intervention, amount of allogeneic blood components administered within 24 hours after start of surgery, and avoidance of red cell transfusions within 24 hours after start of surgery), protocol adherence, and adverse events. The analysis set comprised all randomized patients who had undergone cardiac surgery, received at least 1 dose of either treatment, and provided informed consent after surgery.
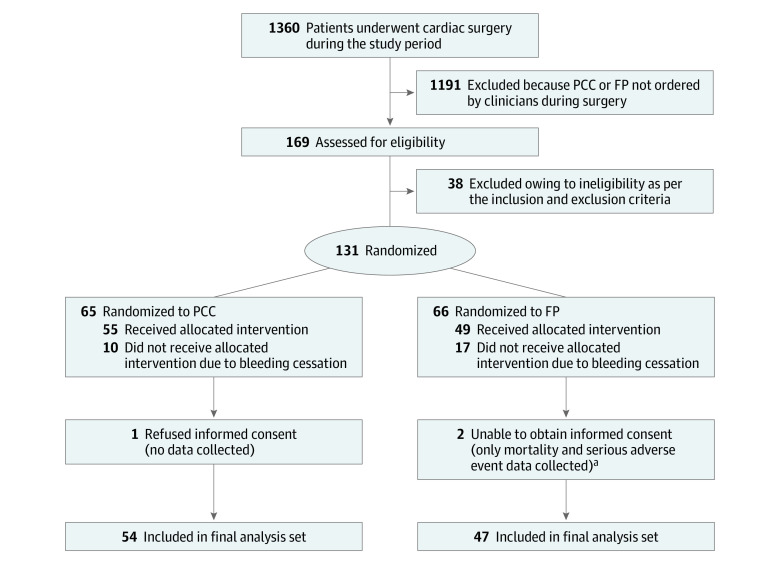
Of 169 screened patients, 131 were randomized, and 101 were treated (54 with PCC and 47 with FP), provided consent, and were included in the analysis (median age, 64 years; interquartile range [IQR], 54-73 years; 28 [28%] were female; 82 [81%] underwent complex operations). The PCC group received a median 24.9 IU/kg (IQR, 21.8-27.0 IU/kg) of PCC (2 patients [3.7%; 95% CI, 0.4%-12.7%] required FP). The FP group received a median 12.5 mL/kg (IQR, 10.0-15.0 mL/kg) of FP (4 patients [8.5%; 95% CI, 2.4%-20.4%] required >2 doses of FP). Hemostatic therapy was not required at the 4-hour time point for 43 patients (80%) in the PCC group and for 32 patients (68%) in the FP group (P = .25) nor at the 24-hour time point for 41 patients (76%) in the PCC group and for 31 patients (66%) patients in the FP group (P = .28). The median numbers of units for 24-hour cumulative allogeneic transfusions (red blood cells, platelets, and FP) were 6.0 U (IQR, 4.0-11.0 U) in the PCC group and 14.0 U (IQR, 8.0-20.0 U) in the FP group (ratio, 0.58; 95% CI, 0.45-0.77; P < .001). After exclusion of FP administered as part of the investigational medicinal product, the median numbers of units were 6.0 U (IQR, 4.0-11.0 U) in the PCC group and 10.0 U (IQR, 6.0-16.0 U) in the FP group (ratio, 0.80; 95% CI, 0.59-1.08; P = .15). For red blood cells alone, the median numbers were 1.5 U (IQR, 0.0-4.0 U) in the PCC group and 3.0 U (IQR, 1.0-5.0 U) in the FP group (ratio, 0.69; 95% CI, 0.47-0.99; P = .05). During the first 24 hours after start of surgery, 15 patients in the PCC group (28%) and 8 patients in the FP group (17%) received no red blood cells (P = .24). Adverse event profiles were similar.
This randomized clinical trial found that the study protocols were feasible. Adequately powered randomized clinical trials are warranted to determine whether PCC is a suitable substitute for FP for mitigation of bleeding in cardiac surgery.
ClinicalTrials.gov Identifier: NCT04114643.
大约 15%接受心脏手术的患者会因出血而输注冷冻血浆 (FP)。四因子凝血酶原复合物浓缩物 (PCC) 在物流和安全性方面优于 FP,可能是一种合适的替代物。
确定接受 PCC 然后需要 FP 的患者比例,探讨止血效果和安全性,并评估研究程序的可行性。
设计、地点和参与者:在加拿大的 2 家医院进行的平行组随机试点研究。成人患者在心脏手术期间因出血需要凝血因子替代治疗(从 2019 年 9 月 23 日至 2020 年 6 月 19 日;最后一次 28 天随访,2020 年 7 月 17 日)。数据分析于 2020 年 9 月 15 日开始。
给予凝血酶原复合物浓缩物(体重≤60 kg 的患者给予 1500 IU,体重>60 kg 的患者给予 2000 IU)或 FP(体重≤60 kg 的患者给予 3 U,体重>60 kg 的患者给予 4 U),在 24 小时内按需重复一次(两组均在后续剂量中使用 FP)。患者和结果评估者对治疗分配不知情。
止血效果(从干预开始后 60 分钟到 4 小时和 24 小时,开始手术后 24 小时内给予的同种异体血液成分的量,以及开始手术后 24 小时内避免红细胞输注)、方案依从性和不良事件。分析集包括所有接受过心脏手术、至少接受过 1 次治疗且术后同意的随机患者。
在筛选的 169 名患者中,131 名被随机分组,101 名接受了治疗(54 名接受 PCC,47 名接受 FP)、同意并被纳入分析(中位年龄 64 岁;四分位距 [IQR],54-73 岁;28 [28%]为女性;82 [81%] 接受复杂手术)。PCC 组接受了中位数为 24.9 IU/kg(IQR,21.8-27.0 IU/kg)的 PCC(2 名患者[3.7%];95%CI,0.4%-12.7%]需要 FP)。FP 组接受了中位数 12.5 mL/kg(IQR,10.0-15.0 mL/kg)的 FP(4 名患者[8.5%];95%CI,2.4%-20.4%]需要>2 剂 FP)。在 PCC 组中,43 名患者(80%)在 4 小时时间点和 41 名患者(76%)在 24 小时时间点无需进行止血治疗(P = .25),在 FP 组中,32 名患者(68%)在 4 小时时间点和 31 名患者(66%)在 24 小时时间点无需进行止血治疗(P = .28)。在 PCC 组中,24 小时累积同种异体输血(红细胞、血小板和 FP)的中位数为 6.0 U(IQR,4.0-11.0 U),在 FP 组中为 14.0 U(IQR,8.0-20.0 U)(比值,0.58;95%CI,0.45-0.77;P < .001)。在排除作为研究药物一部分给予的 FP 后,PCC 组的中位数为 6.0 U(IQR,4.0-11.0 U),FP 组为 10.0 U(IQR,6.0-16.0 U)(比值,0.80;95%CI,0.59-1.08;P = .15)。对于红细胞单独输注,PCC 组的中位数为 1.5 U(IQR,0.0-4.0 U),FP 组的中位数为 3.0 U(IQR,1.0-5.0 U)(比值,0.69;95%CI,0.47-0.99;P = .05)。在手术开始后的前 24 小时内,PCC 组中有 15 名患者(28%)和 FP 组中有 8 名患者(17%)未接受红细胞输注(P = .24)。不良事件谱相似。
这项随机临床试验发现,研究方案是可行的。需要进行充分的、基于人群的随机临床试验,以确定 PCC 是否是心脏手术中出血时替代 FP 的合适替代物。
ClinicalTrials.gov 标识符:NCT04114643。