Knowledge Integration and Translational Platform (KnIT) at Centre for Health Research and Development, Society for Applied Studies, 45, Kalu Sarai, New Delhi, 110016, India.
Centre for Intervention Science in Maternal and Child Health, Centre for International Health, University of Bergen, Bergen, Norway.
BMC Pediatr. 2021 Apr 1;21(1):158. doi: 10.1186/s12887-021-02629-9.
Weight for length z-score (WLZ) < - 3 is currently used to define severe acute malnutrition (SAM) among infants. However, this approach has important limitations for infants younger than 6 months of age as WLZ cannot be calculated using WHO growth standards if infant length is < 45 cm. Moreover, length for age z-score (LAZ) and weight for length z-score (WLZ) are least reliable measures, with high chances of variation, and less chances of detecting undernutrition in under 6 months infants. The objective of the current analysis was to compare WLZ with WAZ and LAZ in a cohort of Indian infants in predicting the deaths between 6 weeks and 6 months of age.
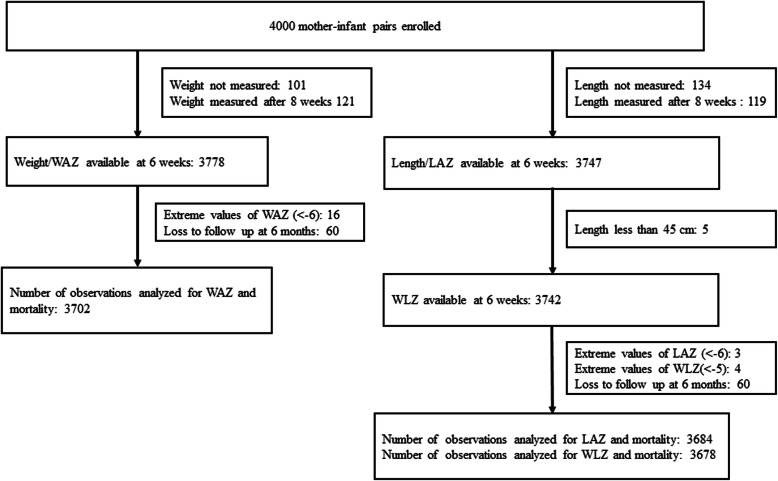
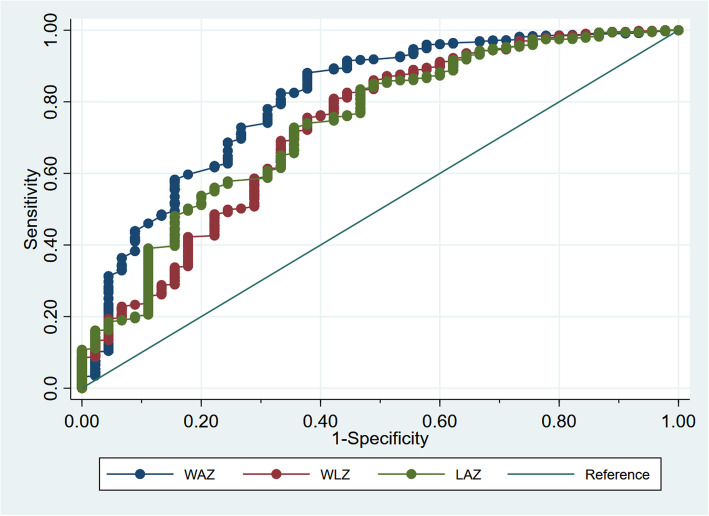
The data was from an individually randomized trial conducted in slums of Delhi, India in which infants' weight and length were measured at 6 weeks of age (at the time of the first immunization visit). Vital status of the infants was documented from 6 weeks to 6 months of age. The sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios were calculated for WAZ < -3, WLZ < -3, and LAZ < -3 for deaths between 6 weeks and 6 months of age. The receiver operating characteristics curve was calculated for each of the above anthropometric indicators.
For deaths occurring between 6 weeks to 6 months of age, the specificity ranged between 85.9-95.9% for all three anthropometric indicators. However, the sensitivity was considerably higher for WAZ; it was 64.6% for WAZ < -3, 39.1% for LAZ < -3, and 25.0% for WLZ < -3. WAZ < -3 had higher area under curve (0.75; 95% CI: 0.68, 0.82) and hence, better discriminated deaths between 6 weeks and 6 months of age than WLZ < -3. The adjusted relative risk (RR 10.6, 95% CI 5.9, 18.9) and the population attributable fraction (PAF 57.9, 95% CI 38.8, 71.0%) of mortality was highest for WAZ < -3.
We found WAZ < -3 at 6 weeks of age to be a better predictor of death in the 6 weeks to 6 months of life in comparison to WLZ < -3 and LAZ < -3 and propose that it should be considered to diagnose SAM in this age group.
目前,体重与身长的 Z 评分(WLZ)<-3 用于定义婴儿中的严重急性营养不良(SAM)。然而,对于 6 个月以下的婴儿,这种方法存在重要的局限性,因为如果婴儿的身长<45 厘米,就无法使用世卫组织生长标准计算 WLZ。此外,年龄与身长的 Z 评分(LAZ)和体重与身长的 Z 评分(WLZ)是最不可靠的指标,变异的可能性很高,并且在 6 个月以下的婴儿中检测营养不良的可能性较小。本分析的目的是比较 WLZ 与 WAZ 和 LAZ 在印度婴儿队列中的预测作用,以评估 6 周至 6 个月期间的死亡情况。
该数据来自印度德里贫民窟进行的一项个体随机试验,其中在婴儿 6 周龄(第 1 次免疫接种就诊时)测量体重和身长。从 6 周龄到 6 个月龄记录婴儿的生存状态。计算 WAZ<-3、WLZ<-3 和 LAZ<-3 对 6 周至 6 个月期间死亡的敏感性、特异性、阳性和阴性预测值以及阳性和阴性似然比。计算了上述每个人体测量指标的接收者操作特征曲线。
对于 6 周至 6 个月期间发生的死亡,所有三种人体测量指标的特异性均在 85.9%-95.9%之间。然而,WAZ 的敏感性要高得多;WAZ<-3 的敏感性为 64.6%,LAZ<-3 的敏感性为 39.1%,WLZ<-3 的敏感性为 25.0%。WAZ<-3 的曲线下面积(0.75;95%CI:0.68,0.82)更高,因此,与 WLZ<-3 相比,能更好地区分 6 周至 6 个月期间的死亡。WAZ<-3 的调整后的相对风险(RR 10.6,95%CI 5.9,18.9)和人群归因分数(PAF 57.9,95%CI 38.8,71.0%)最高。
我们发现,与 WLZ<-3 和 LAZ<-3 相比,WAZ<-3 在 6 周龄时是预测 6 周至 6 个月期间死亡的更好指标,并建议将其用于诊断该年龄组的 SAM。