Schmidt Wolf U, Lutz M, Ploner C J, Braun M
Department of Neurology, Charité Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin Institute of Health, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353, Berlin, Germany.
Center for Stroke Research, Charité Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin Institute of Health, Charitéplatz 1, Berlin, 10117, Germany.
J Neurol. 2021 Oct;268(10):3826-3834. doi: 10.1007/s00415-021-10527-4. Epub 2021 Apr 1.
Identifying the cause of non-traumatic coma in the emergency department is challenging. The clinical neurological examination is the most readily available tool to detect focal neurological deficits as indicators for cerebral causes of coma. Previously proposed clinical pathways have granted the interpretation of clinical findings a pivotal role in the diagnostic work-up. We aimed to identify the actual diagnostic reliability of the neurological examination with regard to identifying acute brain damage.
Eight hundred and fifty-three patients with coma of unknown etiology (CUE) were examined neurologically in the emergency department following a predefined routine. Coma-explaining pathologies were identified retrospectively and grouped into primary brain pathology with proof of acute brain damage and other causes without proof of acute structural pathology. Sensitivity, specificity and percentage of correct predictions of different examination protocols were calculated using contingency tables and binary logistic regression models.
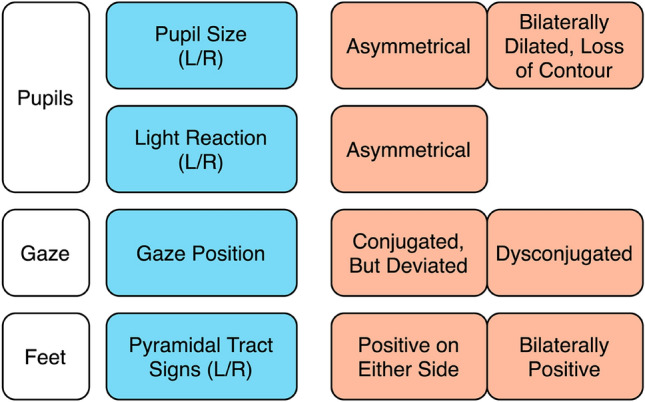
The full neurological examination was 74% sensitive and 60% specific to detect acute structural brain damage underlying CUE. Sensitivity and specificity were higher in non-sedated patients (87/61%) compared to sedated patients (64%/59%). A shortened four-item examination protocol focusing on pupils, gaze and pyramidal tract signs was only slightly less sensitive (67%) and more specific (65%).
Due to limited diagnostic reliability of the physical examination, the absence of focal neurological signs in acutely comatose patients should not defer from a complete work-up including brain imaging. In an emergency, a concise neurological examination should thus serve as one part of a multimodal diagnostic approach to CUE.
在急诊科确定非创伤性昏迷的病因具有挑战性。临床神经学检查是检测局灶性神经功能缺损的最便捷工具,而局灶性神经功能缺损是昏迷脑部病因的指标。先前提出的临床路径赋予了临床检查结果的解读在诊断检查中关键作用。我们旨在确定神经学检查在识别急性脑损伤方面的实际诊断可靠性。
按照预定义的常规流程,对853例病因不明的昏迷(CUE)患者在急诊科进行神经学检查。回顾性确定可解释昏迷的病变,并分为有急性脑损伤证据的原发性脑病变和无急性结构病变证据的其他病因。使用列联表和二元逻辑回归模型计算不同检查方案的敏感性、特异性和正确预测百分比。
全面的神经学检查检测CUE潜在急性结构性脑损伤的敏感性为74%,特异性为60%。与使用镇静剂的患者(64%/59%)相比,未使用镇静剂的患者敏感性(87%)和特异性(61%)更高。一个缩短的四项检查方案,重点关注瞳孔、凝视和锥体束征,敏感性略低(67%)但特异性更高(65%)。
由于体格检查的诊断可靠性有限,急性昏迷患者缺乏局灶性神经体征不应妨碍包括脑成像在内的全面检查。因此,在紧急情况下,简洁的神经学检查应作为CUE多模式诊断方法的一部分。