Cardiology Department, Hospital Clínico San Carlos, Instituto de Investigación Sanitaria del Hospital Clínico San Carlos (IdISSC), Madrid, Spain.
Servicio de Medicina Preventiva, Hospital Clínico San Carlos, Instituto de Investigación Sanitaria San Carlos (IdISSC), Madrid, Spain.
PLoS One. 2021 Apr 2;16(4):e0245898. doi: 10.1371/journal.pone.0245898. eCollection 2021.
We aimed to compare the performance of the recent CASTLE score to J-CTO, CL and PROGRESS CTO scores in a comprehensive database of percutaneous coronary intervention of chronic total occlusion procedures.
Scores were calculated using raw data from 1,342 chronic total occlusion procedures included in REBECO Registry that includes learning and expert operators. Calibration, discrimination and reclassification were evaluated and compared.
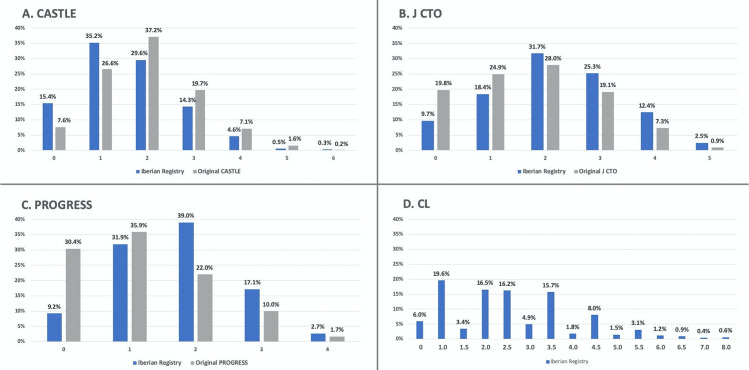
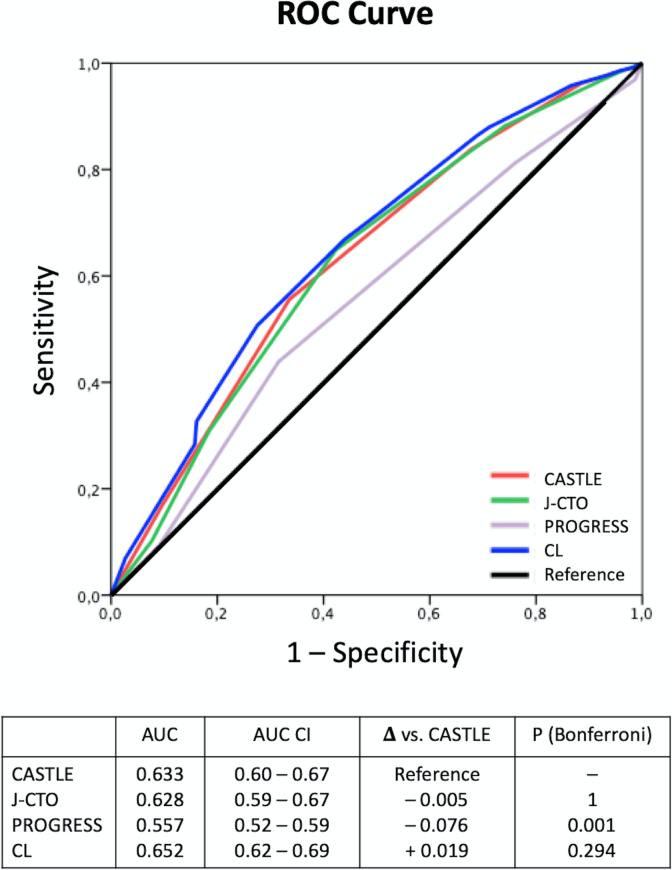
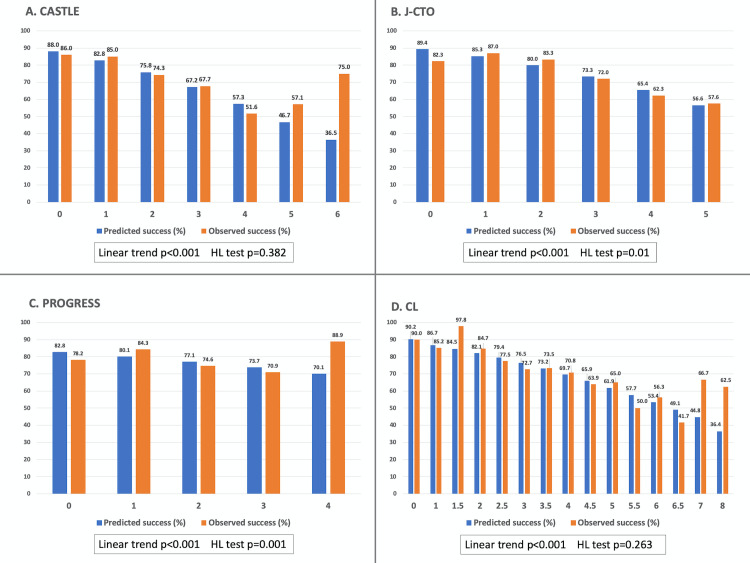
Mean score values were: CASTLE 1.60±1.10, J-CTO 2.15±1.24, PROGRESS 1.68±0.94 and CL 2.52±1.52 points. The overall percutaneous coronary intervention success rate was 77.8%. Calibration was good for CASTLE and CL, but not for J-CTO or PROGRESS scores. Discrimination: the area under the curve (AUC) of CASTLE (0.633) was significantly higher than PROGRESS (0.557) and similar to J-CTO (0.628) and CL (0.652). Reclassification: CASTLE, as assessed by integrated discrimination improvement, was superior to PROGRESS (integrated discrimination improvement +0.036, p<0.001), similar to J-CTO and slightly inferior to CL score (- 0.011, p = 0.004). Regarding net reclassification improvement, CASTLE reclassified better than PROGRESS (overall continuous net reclassification improvement 0.379, p<0.001) in roughly 20% of cases.
Procedural percutaneous coronary intervention difficulty is not consistently depicted by available chronic total occlusion scores and is influenced by the characteristics of each chronic total occlusion cohort. In our study population, including expert and learning operators, the CASTLE score had slightly better overall performance along with CL score. However, we found only intermediate performance in the c-statistic predicting chronic total occlusion success among all scores.
我们旨在比较最近的 CASTLE 评分与 J-CTO、CL 和 PROGRESS CTO 评分在慢性完全闭塞经皮冠状动脉介入治疗综合数据库中的表现。
使用包括学习和专家操作人员在内的 REBECO 登记处纳入的 1342 例慢性完全闭塞病例的原始数据计算评分。评估和比较了校准、区分度和重新分类。
平均评分值分别为:CASTLE 1.60±1.10、J-CTO 2.15±1.24、PROGRESS 1.68±0.94 和 CL 2.52±1.52 分。总的经皮冠状动脉介入治疗成功率为 77.8%。CASTLE 和 CL 的校准良好,但 J-CTO 和 PROGRESS 评分的校准不佳。区分度:CASTLE(0.633)的曲线下面积(AUC)明显高于 PROGRESS(0.557),与 J-CTO(0.628)和 CL(0.652)相似。重新分类:CASTLE 在整体鉴别改善方面优于 PROGRESS(整体鉴别改善+0.036,p<0.001),与 J-CTO 相似,略低于 CL 评分(-0.011,p=0.004)。关于净重新分类改善,CASTLE 在大约 20%的病例中比 PROGRESS 更好地重新分类(总连续净重新分类改善 0.379,p<0.001)。
可用的慢性完全闭塞评分并不能一致地描述手术经皮冠状动脉介入治疗的难度,并且受到每个慢性完全闭塞队列的特征的影响。在我们的研究人群中,包括专家和学习操作人员,CASTLE 评分与 CL 评分的整体表现略好。然而,我们发现所有评分中,预测慢性完全闭塞成功的 C 统计量仅具有中等性能。