Munirwan Haris, Kusyanto Fahmi A, Zanisa Zanisa, Latief Muhammad H
Departement of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Syiah Kuala, Banda Aceh, Indonesia.
Departement of Cardiology and Vascular Medicine, Dr. Zainoel Abidin Hospital, Banda Aceh, Indonesia.
Narra J. 2023 Aug;3(2):e140. doi: 10.52225/narra.v3i2.140. Epub 2023 Jul 12.
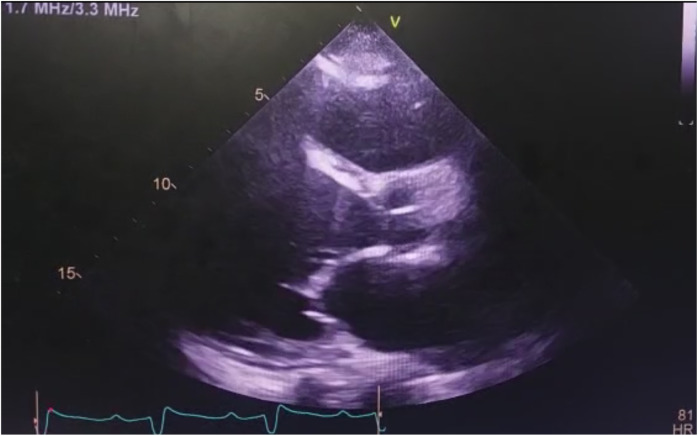
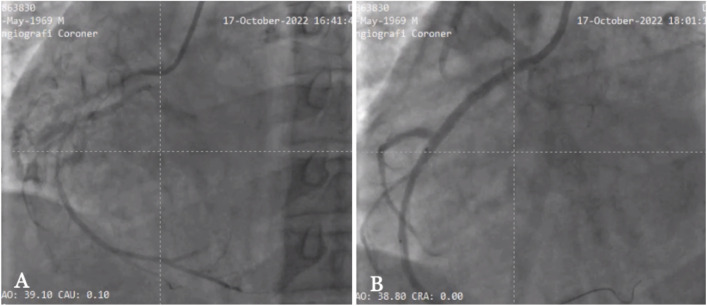
One of the most difficult procedures in interventional cardiology is the percutaneous coronary intervention (PCI) on a chronic total occlusion (CTO) lesion case. To rate the difficulty of guidewire crossing, several angiographic scoring methods have been developed such as the Japan CTO (J-CTO) score. Here we demonstrate the advantages of revascularization using PCI procedure in a CTO case with intractable heart failure. A 53-year-old man presented to the emergency room of Dr. Zainoel Abidin Hospital, Banda Aceh, Indonesia with acute decompensated heart failure. The patient had a history of past PCI with two patent drug eluting stents (DES): one in the left main (LM)-left anterior descending (LAD) artery and one in the distal left circumflex (LCX) artery. The patient had three times rehospitalizations in the last three months. According to single-photon emission computed tomography (SPECT) imaging, the right coronary artery was remained functional; however, the lesion was categorized into very difficult level (J-CTO >3). The PCI was carried out on the right coronary artery and the blood vessel was successfully revascularized after applying multiple techniques. Following the procedure, the heart failure was treated and the 6-minute walking test (6MWT) that performed 12 days after the PCI increased from 220 to 260 meters. The success of this case depended on a comprehensive history taking, adequate imaging methods, and the selection of the proper tools and PCI strategy. In conclusion, despite the challenges, PCI is still an option for patients with persistent complete occlusion. The PCI requires comprehensive preparation and the use of angiographic scoring systems, such as the J-CTO score, to determine the approach and the likelihood of success.
介入心脏病学中最具挑战性的操作之一是针对慢性完全闭塞(CTO)病变病例进行经皮冠状动脉介入治疗(PCI)。为了评估导丝通过的难度,已经开发了多种血管造影评分方法,如日本CTO(J-CTO)评分。在此,我们展示了在一例伴有顽固性心力衰竭的CTO病例中使用PCI进行血运重建的优势。一名53岁男性因急性失代偿性心力衰竭被送往印度尼西亚班达亚齐宰诺埃尔·阿比丁博士医院的急诊室。该患者既往有PCI病史,植入了两枚药物洗脱支架(DES):一枚位于左主干(LM)-左前降支(LAD)动脉,另一枚位于左旋支(LCX)动脉远端。该患者在过去三个月内三次住院。根据单光子发射计算机断层扫描(SPECT)成像,右冠状动脉仍有功能;然而,该病变被归类为极难级别(J-CTO>3)。在右冠状动脉上进行了PCI,应用多种技术后血管成功实现血运重建。术后,对心力衰竭进行了治疗,PCI术后12天进行的6分钟步行试验(6MWT)从220米增加到了260米。该病例的成功取决于全面的病史采集、充分的成像方法以及合适工具和PCI策略的选择。总之,尽管存在挑战,但PCI仍是持续性完全闭塞患者的一种选择。PCI需要全面的准备,并使用血管造影评分系统,如J-CTO评分,来确定治疗方法和成功的可能性。