National Diabetes Audit Programme, NHS England & Improvement, London, UK; Leicester Real World Evidence Unit, Diabetes Research Centre, University of Leicester, Leicester General Hospital, Leicester, UK.
National Diabetes Audit Programme, NHS England & Improvement, London, UK; NHS Digital, Leeds, UK.
Lancet Diabetes Endocrinol. 2021 May;9(5):293-303. doi: 10.1016/S2213-8587(21)00050-4. Epub 2021 Mar 30.
In patients with type 2 diabetes, hyperglycaemia is an independent risk factor for COVID-19-related mortality. Associations between pre-infection prescription for glucose-lowering drugs and COVID-19-related mortality in people with type 2 diabetes have been postulated but only investigated in small studies and limited to a few agents. We investigated whether there are associations between prescription of different classes of glucose-lowering drugs and risk of COVID-19-related mortality in people with type 2 diabetes.
This was a nationwide observational cohort study done with data from the National Diabetes Audit for people with type 2 diabetes and registered with a general practice in England since 2003. Cox regression was used to estimate the hazard ratio (HR) of COVID-19-related mortality in people prescribed each class of glucose-lowering drug, with covariate adjustment with a propensity score to address confounding by demographic, socioeconomic, and clinical factors.
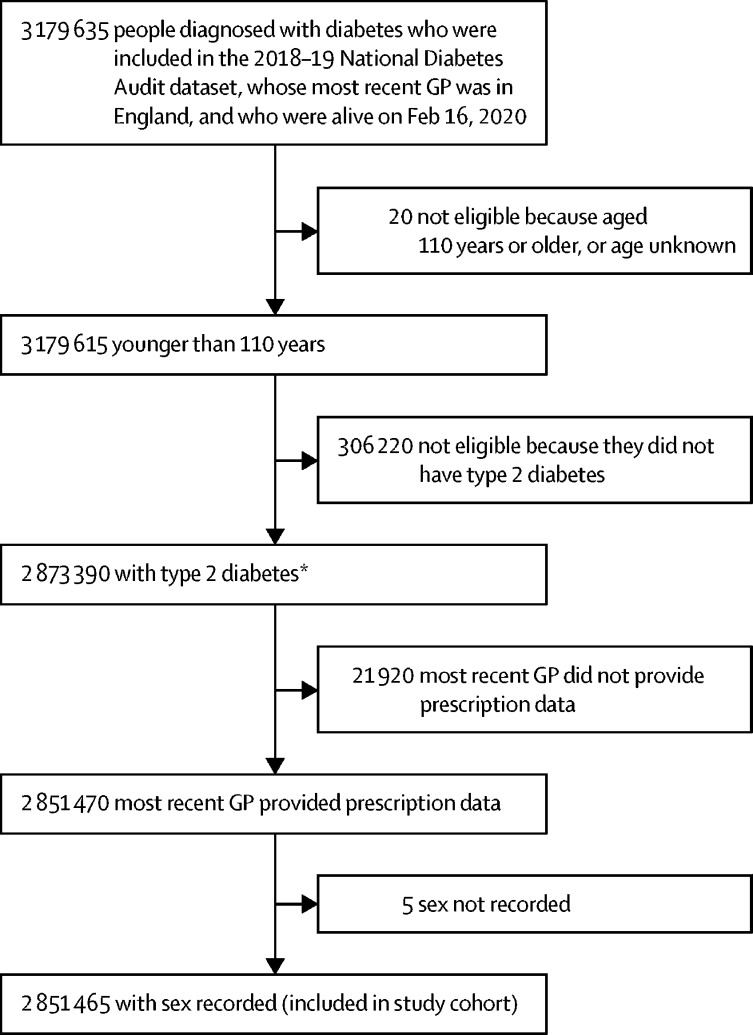
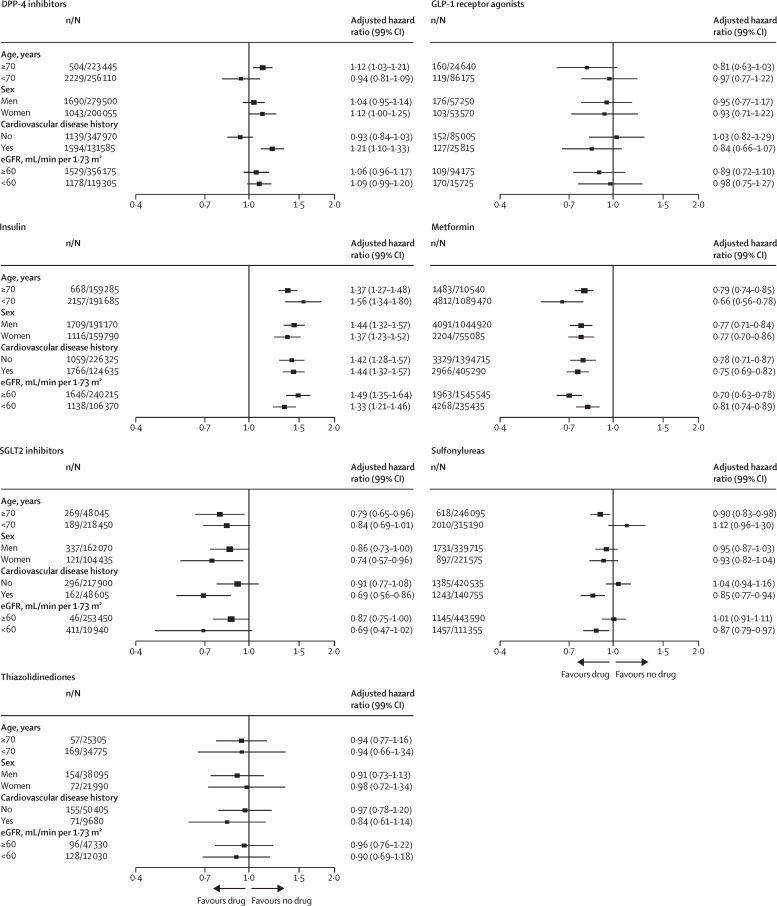
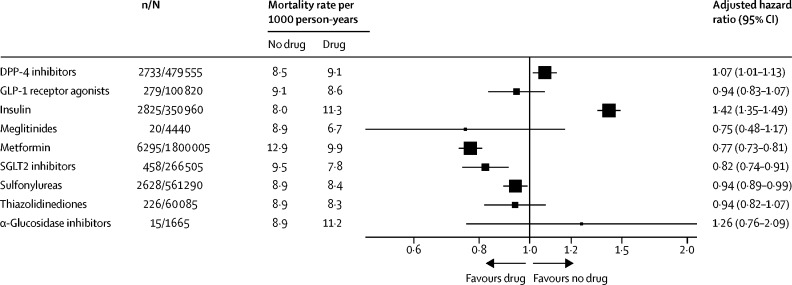
Among the 2 851 465 people with type 2 diabetes included in our analyses, 13 479 (0·5%) COVID-19-related deaths occurred during the study period (Feb 16 to Aug 31, 2020), corresponding to a rate of 8·9 per 1000 person-years (95% CI 8·7-9·0). The adjusted HR associated with recorded versus no recorded prescription was 0·77 (95% CI 0·73-0·81) for metformin and 1·42 (1·35-1·49) for insulin. Adjusted HRs for prescription of other individual classes of glucose-lowering treatment were as follows: 0·75 (0·48-1·17) for meglitinides, 0·82 (0·74-0·91) for SGLT2 inhibitors, 0·94 (0·82-1·07) for thiazolidinediones, 0·94 (0·89-0·99) for sulfonylureas, 0·94 (0·83-1·07) for GLP-1 receptor agonists, 1·07 (1·01-1·13) for DPP-4 inhibitors, and 1·26 (0·76-2·09) for α-glucosidase inhibitors.
Our results provide evidence of associations between prescription of some glucose-lowering drugs and COVID-19-related mortality, although the differences in risk are small and these findings are likely to be due to confounding by indication, in view of the use of different drug classes at different stages of type 2 diabetes disease progression. In the context of the COVID-19 pandemic, there is no clear indication to change prescribing of glucose-lowering drugs in people with type 2 diabetes.
None.
在 2 型糖尿病患者中,高血糖是 COVID-19 相关死亡的独立危险因素。有人推测,感染前开具的降糖药物与 2 型糖尿病患者的 COVID-19 相关死亡率之间存在关联,但这些关联仅在小型研究中进行了调查,且仅局限于几种药物。我们调查了不同类别的降糖药物处方与 2 型糖尿病患者 COVID-19 相关死亡率之间是否存在关联。
这是一项全国性观察性队列研究,数据来自自 2003 年以来在英格兰接受过 2 型糖尿病国家糖尿病审计且在普通诊所登记的患者。使用 Cox 回归来估计处方中每类降糖药物与 COVID-19 相关死亡率的风险比(HR),通过倾向评分进行协变量调整,以解决人口统计学、社会经济学和临床因素造成的混杂。
在我们的分析中,纳入了 2851465 名 2 型糖尿病患者,研究期间(2020 年 2 月 16 日至 8 月 31 日)发生了 13479 例(0.5%)COVID-19 相关死亡,相应的死亡率为每 1000 人年 8.9 例(95%CI 8.7-9.0)。与有记录处方与无记录处方相比,记录处方与无记录处方的调整 HR 为 0.77(95%CI 0.73-0.81),而胰岛素的调整 HR 为 1.42(1.35-1.49)。其他个别类别的降糖治疗处方的调整 HR 如下:格列奈类为 0.75(0.48-1.17),SGLT2 抑制剂为 0.82(0.74-0.91),噻唑烷二酮类为 0.94(0.89-0.99),磺脲类为 0.94(0.83-1.07),GLP-1 受体激动剂为 0.94(0.83-1.07),DPP-4 抑制剂为 1.07(1.01-1.13),α-葡萄糖苷酶抑制剂为 1.26(0.76-2.09)。
我们的结果提供了一些降糖药物处方与 COVID-19 相关死亡率之间存在关联的证据,尽管风险差异较小,而且考虑到在 2 型糖尿病疾病进展的不同阶段使用不同的药物类别,这些发现很可能归因于混杂因素。在 COVID-19 大流行背景下,没有明确的证据表明需要改变 2 型糖尿病患者的降糖药物处方。
无。