Schavemaker Renée, Schultz Marcus J, Lagrand Wim K, van Slobbe-Bijlsma Eline R, Serpa Neto Ary, Paulus Frederique
Department of Intensive Care, Amsterdam UMC, Location AMC, 1105 AZ Amsterdam, The Netherlands.
Mahidol Oxford Tropical Medicine Research Unit (MORU), Mahidol University, Bangkok 10400, Thailand.
J Clin Med. 2021 Mar 11;10(6):1176. doi: 10.3390/jcm10061176.
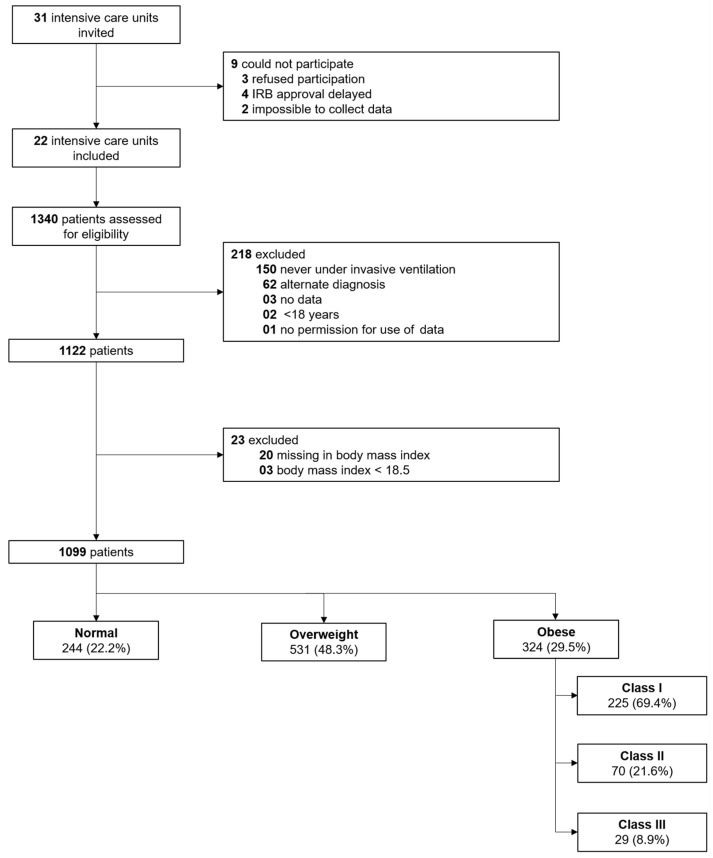
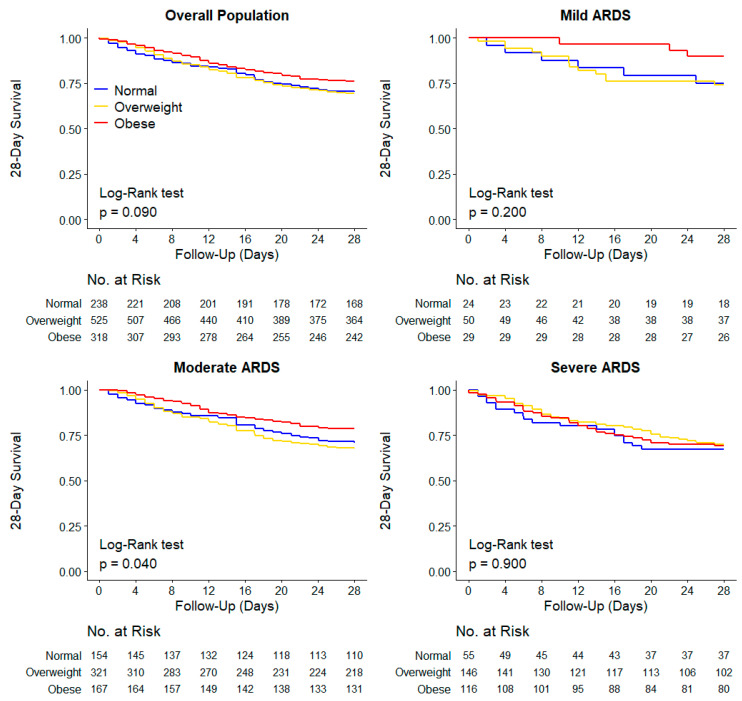
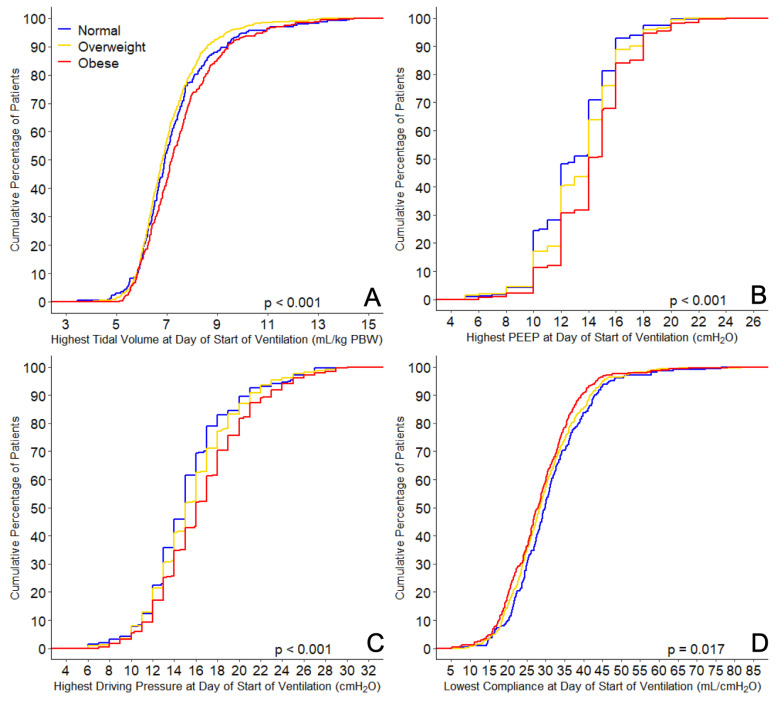
We describe the practice of ventilation and mortality rates in invasively ventilated normal-weight (18.5 ≤ BMI ≤ 24.9 kg/m), overweight (25.0 ≤ BMI ≤ 29.9 kg/m), and obese (BMI > 30 kg/m) COVID-19 ARDS patients in a national, multicenter observational study, performed at 22 intensive care units in the Netherlands. The primary outcome was a combination of ventilation variables and parameters over the first four calendar days of ventilation, including tidal volume, positive end-expiratory pressure (PEEP), respiratory system compliance, and driving pressure in normal-weight, overweight, and obese patients. Secondary outcomes included the use of adjunctive treatments for refractory hypoxaemia and mortality rates. Between 1 March 2020 and 1 June 2020, 1122 patients were included in the study: 244 (21.3%) normal-weight patients, 531 (47.3%) overweight patients, and 324 (28.8%) obese patients. Most patients received a tidal volume < 8 mL/kg PBW; only on the first day was the tidal volume higher in obese patients. PEEP and driving pressure were higher, and compliance of the respiratory system was lower in obese patients on all four days. Adjunctive therapies for refractory hypoxemia were used equally in the three BMI groups. Adjusted mortality rates were not different between BMI categories. The findings of this study suggest that lung-protective ventilation with a lower tidal volume and prone positioning is similarly feasible in normal-weight, overweight, and obese patients with ARDS related to COVID-19. A patient's BMI should not be used in decisions to forgo or proceed with invasive ventilation.
在荷兰22家重症监护病房进行的一项全国性多中心观察性研究中,我们描述了有创通气的正常体重(18.5≤体重指数[BMI]≤24.9kg/m²)、超重(25.0≤BMI≤29.9kg/m²)和肥胖(BMI>30kg/m²)的新型冠状病毒肺炎急性呼吸窘迫综合征(COVID-19 ARDS)患者的通气实践和死亡率。主要结局是通气头四个日历日的通气变量和参数组合,包括潮气量、呼气末正压(PEEP)、呼吸系统顺应性以及正常体重、超重和肥胖患者的驱动压。次要结局包括对难治性低氧血症的辅助治疗使用情况和死亡率。在2020年3月1日至2020年6月1日期间,1122例患者纳入研究:244例(21.3%)正常体重患者、531例(47.3%)超重患者和324例(28.8%)肥胖患者。大多数患者接受的潮气量<8mL/kg预计体重;仅在第一天肥胖患者的潮气量较高。在所有四天中,肥胖患者的PEEP和驱动压较高,而呼吸系统顺应性较低。三个BMI组对难治性低氧血症的辅助治疗使用情况相同。BMI类别之间的校正死亡率无差异。本研究结果表明,对于与COVID-19相关的ARDS,正常体重、超重和肥胖患者采用较低潮气量和俯卧位的肺保护性通气同样可行。在决定是否放弃或进行有创通气时,不应考虑患者的BMI。