Park Sohyun, Choi Yeo Jin, Kang Ji Eun, Kim Myeong Gyu, Jung Geum Min, Kim So Dam, Rhie Sandy Jeong
Division of Life and Pharmaceutical Sciences Graduate School, Ewha Womans University, Seoul 03760, Korea.
Department of Pharmacy, National Medical Center, Seoul 04564, Korea.
J Pers Med. 2021 Mar 21;11(3):222. doi: 10.3390/jpm11030222.
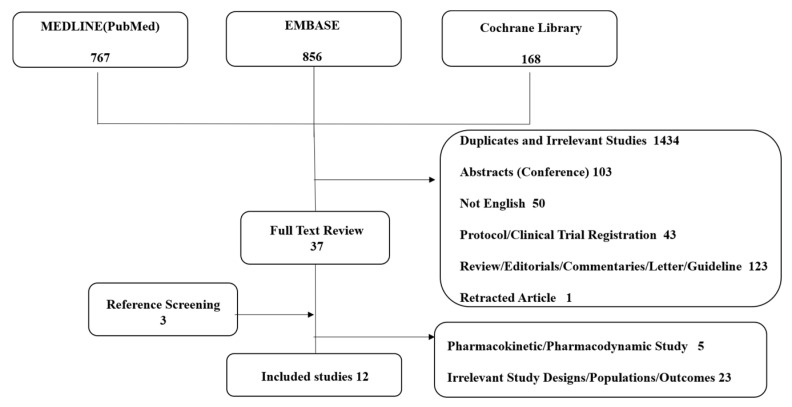
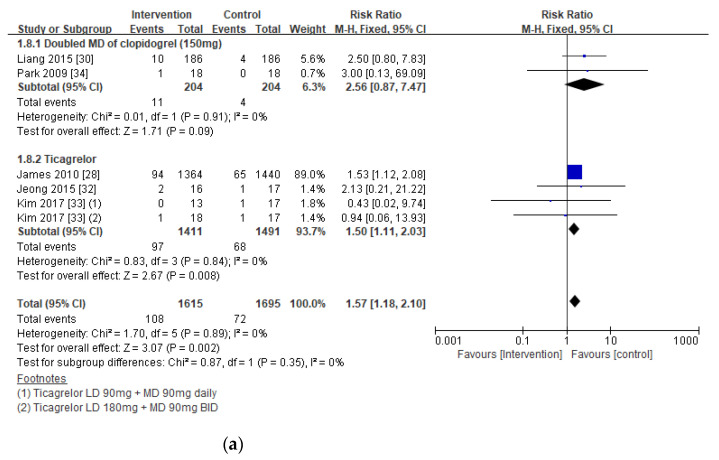
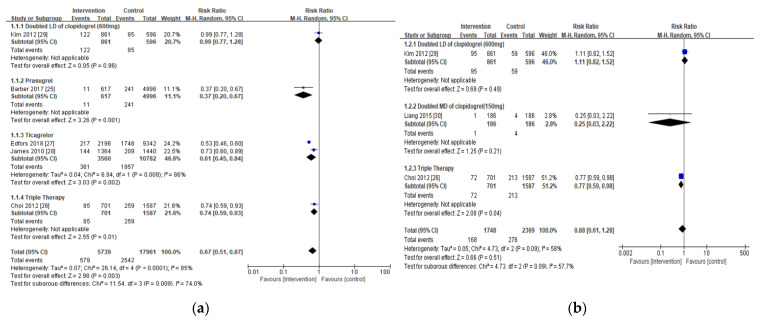
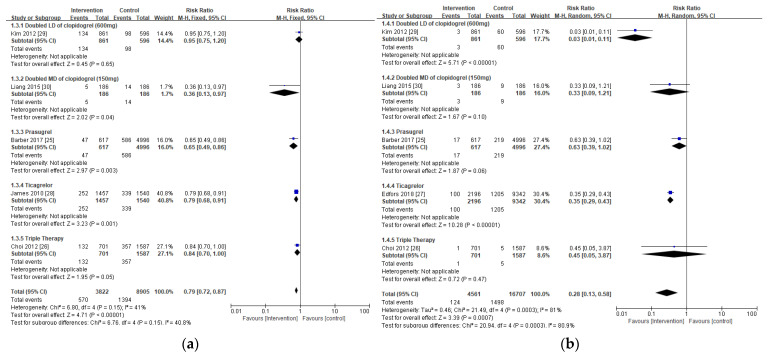
This study aims to evaluate potentially appropriate antiplatelet therapy in patients with chronic kidney disease. A systematic analysis was conducted to identify the clinical outcomes of available antiplatelet therapy regimens with enhanced platelet inhibition activity (intervention of 5 regimens) over the standard dose of clopidogrel-based dual antiplatelet therapy in patients with renal insufficiency. An electronic keyword search was performed on Pubmed, Embase, and Cochrane Library per PRISMA guidelines. We performed a prespecified net clinical benefit analysis (a composite of the rates of all-cause or cardiac-related death, myocardial infarction, major adverse cardiac outcomes, and minor and major bleeding), and included 12 studies. The intervention substantially lowered the incidence of all-cause mortality (RR 0.67; = 0.003), major adverse cardiac outcomes (RR 0.79; < 0.00001), and myocardial infarction (RR 0.28; = 0.00007) without major bleeding (RR 1.14; = 0.33) in patients with renal insufficiency, but no significant differences were noticed with cardiac-related mortality and stent thrombosis. The subgroup analysis revealed substantially elevated bleeding risk in patients with severe renal insufficiency or on hemodialysis (RR 1.68; = 0.002). Our study confirmed that the intervention considerably enhances clinical outcomes in patients with renal insufficiency, however, a standard dose of clopidogrel-based antiplatelet therapy is favorable in patients with severe renal insufficiency.
本研究旨在评估慢性肾脏病患者潜在合适的抗血小板治疗。进行了一项系统分析,以确定在肾功能不全患者中,与基于氯吡格雷的标准剂量双联抗血小板治疗相比,具有增强血小板抑制活性的现有抗血小板治疗方案(5种方案的干预)的临床结局。根据PRISMA指南,在PubMed、Embase和Cochrane图书馆进行了电子关键词搜索。我们进行了预先设定的净临床获益分析(全因死亡或心脏相关死亡、心肌梗死、主要不良心脏结局以及轻微和严重出血发生率的综合指标),纳入了12项研究。该干预措施显著降低了肾功能不全患者的全因死亡率(RR 0.67; = 0.003)、主要不良心脏结局(RR 0.79; < 0.00001)和心肌梗死发生率(RR 0.28; = 0.00007),且未出现严重出血(RR 1.14; = 0.33),但在心脏相关死亡率和支架血栓形成方面未观察到显著差异。亚组分析显示,严重肾功能不全或接受血液透析的患者出血风险显著升高(RR 1.68; = 0.002)。我们的研究证实,该干预措施可显著改善肾功能不全患者的临床结局,然而,对于严重肾功能不全患者,基于氯吡格雷的标准剂量抗血小板治疗是有利的。