Semaan Carl, Charbonnier Arthur, Pasco Jeremy, Darwiche Walid, Saint Etienne Christophe, Bailleul Xavier, Bourguignon Thierry, Fauchier Laurent, Angoulvant Denis, Ivanes Fabrice, Genet Thibaud
Service de Cardiologie, Centre Hospitalier Régional, Universitaire de Tours, 37044 Tours, France.
Faculté de Médecine, Université de Tours, 37032 Tours, France.
J Clin Med. 2021 Mar 1;10(5):956. doi: 10.3390/jcm10050956.
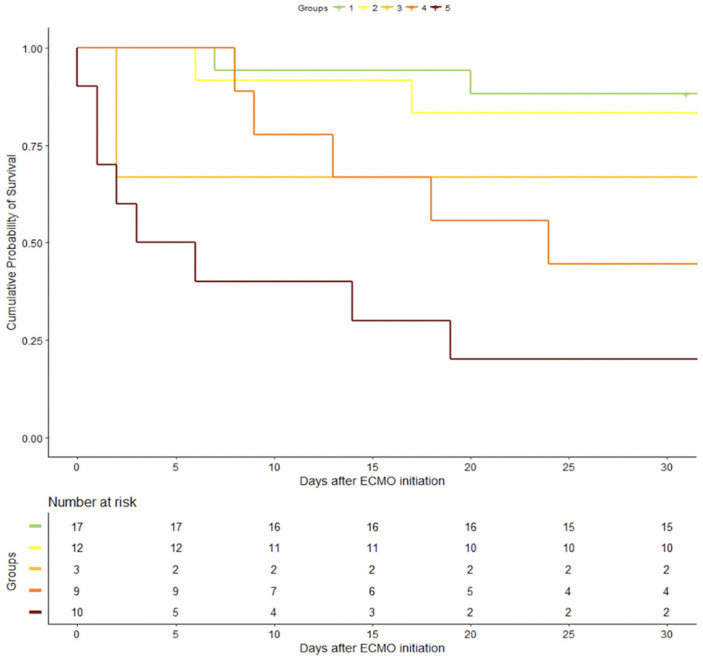
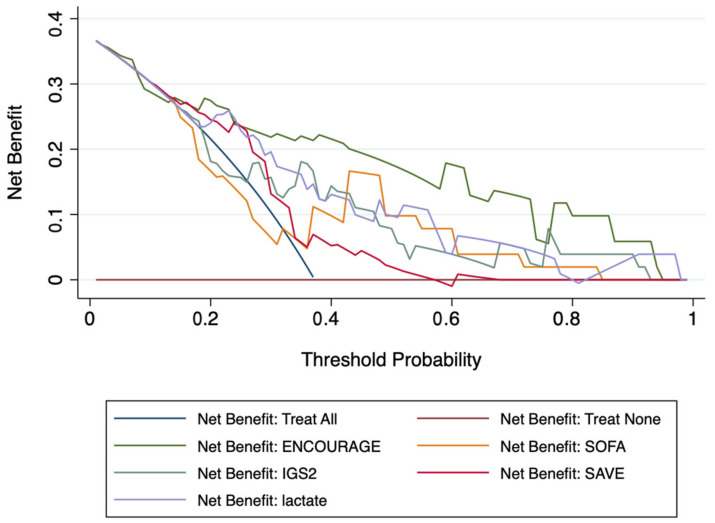
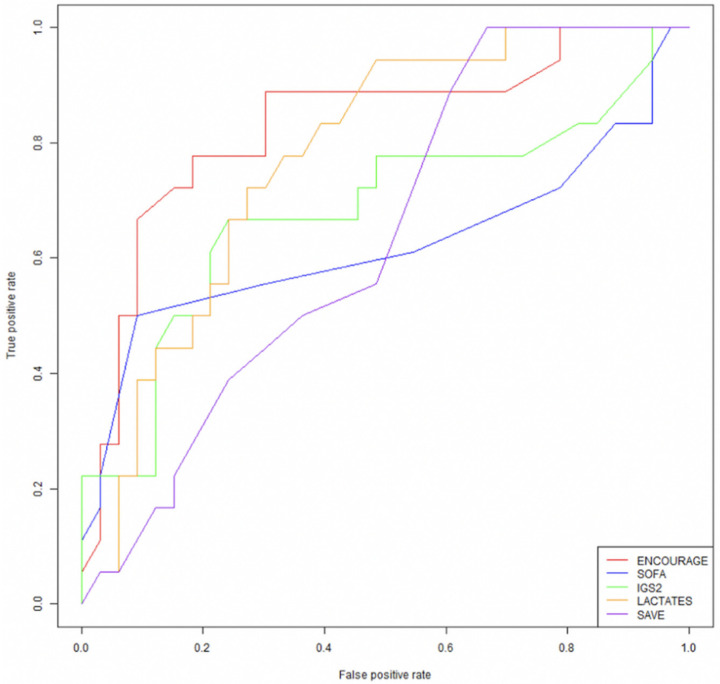
Although many risk models have been tested in patients implanted by veno-arterial extracorporeal membrane oxygenation (VA-ECMO), few scores assessed patients' prognosis in the setting of ST-segment elevation myocardial infarction (STEMI) with refractory cardiogenic shock. We aimed at assessing the performance of risk scores, notably the prEdictioN of Cardiogenic shock OUtcome foR AMI patients salvaGed by VA-ECMO (ENCOURAGE) score, for predicting mortality in this particular population. This retrospective observational study included patients admitted to Tours University Hospital for STEMI with cardiogenic shock and requiring hemodynamic support by VA-ECMO. Among the fifty-one patients, the 30-day and 6-month survival rates were 63% and 56% respectively. Thirty days after VA-ECMO therapy, probabilities of mortality were 12, 17, 33, 66, 80% according to the ENCOURAGE score classes 0-12, 13-18, 19-22, 23-27, and ≥28, respectively. The ENCOURAGE score (AUC of the Receiving Operating Characteristic curve = 0.83) was significantly better compared to other risk scores. The hazard ratio for survival at 30 days for each point of the ENCOURAGE score was 1.10 (CI 95% (1.06, 1.15); < 0.001). Decision curve analysis indicated that the ENCOURAGE score had the best clinical usefulness of the tested risk scores and the Hosmer-Lemeshow test suggested an accurate calibration. Our data suggest that the ENCOURAGE score is valid and the most relevant score to predict 30-day mortality after VA-ECMO therapy in STEMI patients with refractory cardiogenic shock. It may help decision-making teams to better select STEMI patients with shock for VA-ECMO therapy.
尽管许多风险模型已在接受静脉-动脉体外膜肺氧合(VA-ECMO)植入的患者中进行了测试,但很少有评分系统评估过ST段抬高型心肌梗死(STEMI)合并难治性心源性休克患者的预后。我们旨在评估风险评分系统,尤其是用于预测VA-ECMO挽救的急性心肌梗死(AMI)患者心源性休克结局的预测评分(ENCOURAGE评分),对这一特定人群死亡率的预测性能。这项回顾性观察性研究纳入了因STEMI合并心源性休克而入住图尔大学医院且需要VA-ECMO进行血流动力学支持的患者。在这51例患者中,30天和6个月生存率分别为63%和56%。VA-ECMO治疗30天后 根据ENCOURAGE评分等级0-12、13-18、19-22、23-27和≥28,死亡率概率分别为12%、17%、33%、66%、80%。与其他风险评分相比,ENCOURAGE评分(受试者工作特征曲线下面积=0.83)明显更好。ENCOURAGE评分每增加1分,30天生存的风险比为1.10(95%置信区间(1.06,1.15);P<0.001)。决策曲线分析表明,ENCOURAGE评分在测试的风险评分中具有最佳的临床实用性,Hosmer-Lemeshow检验表明校准准确。我们的数据表明,ENCOURAGE评分是有效的,并且是预测VA-ECMO治疗后STEMI合并难治性心源性休克患者3日死亡率最相关的评分。它可能有助于决策团队更好地选择适合VA-ECMO治疗的STEMI休克患者。