Immunoallergology Unit, University Hospital Careggi, 50134 Florence, Italy.
Immunology and Cellular Therapy Unit, University Hospital Careggi, 50134 Florence, Italy.
Int J Mol Sci. 2021 Mar 24;22(7):3340. doi: 10.3390/ijms22073340.
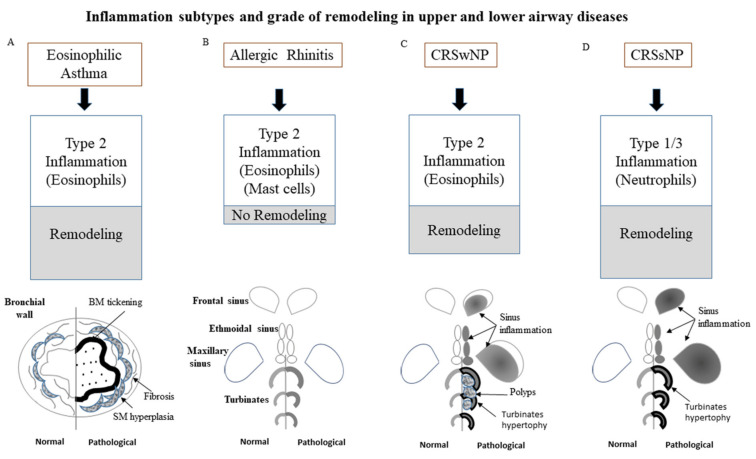
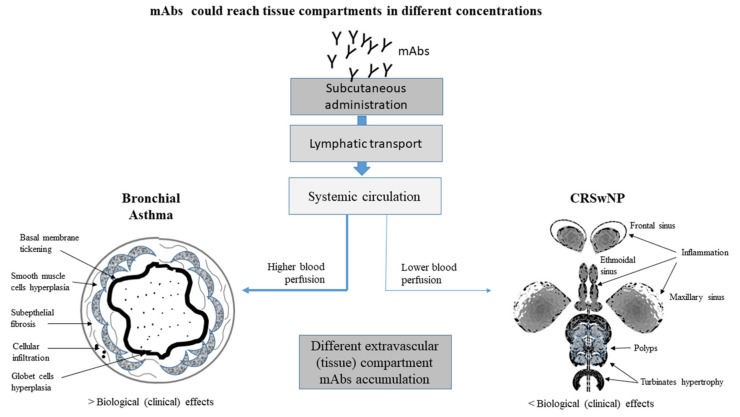
Severe asthma and rhinosinusitis represent frequent comorbidities, complicating the overall management of the disease. Both asthma and chronic rhinosinusitis (CRS) can be differentiated into endotypes: those with type 2 eosinophilic inflammation and those with a non-type 2 inflammation. A correct definition of phenotype/endotype for these diseases is crucial, taking into account the availability of novel biological therapies. Even though patients suffering from type 2 severe asthma-with or without CRS with nasal polyps-significantly benefit from treatment with biologics, the existence of different levels of patient response has been clearly demonstrated. In fact, in clinical practice, it is a common experience that patients reach a good clinical response for asthma symptoms, but not for CRS. At first glance, a reason for this could be that although asthma and CRS can coexist in the same patient, they can manifest with different degrees of severity; therefore, efficacy may not be equally achieved. Many questions regarding responders and nonresponders, predictors of response, and residual disease after blocking type 2 pathways are still unanswered. In this review, we discuss whether treatment with biological agents is equally effective in controlling both asthma and sinonasal symptoms in patients in which asthma and chronic rhinosinusitis with nasal polyps coexist.
严重哮喘和鼻-鼻窦炎常合并存在,使疾病的整体管理复杂化。哮喘和慢性鼻-鼻窦炎(CRS)都可以分为表型/内型:2 型嗜酸性粒细胞炎症型和非 2 型炎症型。对于这些疾病,正确定义表型/内型至关重要,要考虑到新型生物疗法的应用。尽管接受生物制剂治疗的 2 型重度哮喘(无论是否合并有鼻息肉的 CRS)患者获益显著,但患者的反应存在明显差异。事实上,在临床实践中,我们常遇到患者的哮喘症状得到了很好的临床缓解,但 CRS 却没有的情况。乍一看,这可能是因为尽管哮喘和 CRS 可以同时存在于同一患者中,但它们可能表现出不同程度的严重程度;因此,疗效可能无法同等实现。许多关于应答者和无应答者、反应预测因子以及阻断 2 型通路后残余疾病的问题仍未得到解答。在这篇综述中,我们讨论了在同时患有哮喘和鼻息肉的慢性鼻-鼻窦炎的患者中,生物制剂治疗是否同样能有效控制哮喘和鼻-鼻窦症状。