Delanoy Nicolas, Robbrecht Debbie, Eisenberger Mario, Sartor Oliver, de Wit Ronald, Mercier Florence, Geffriaud-Ricouard Christine, de Bono Johann, Oudard Stéphane
Medical Oncology, Université de Paris, 75015 Paris, France.
Medical Oncology, AP-HP Paris, Centre, Georges Pompidou European Hospital, 75015 Paris, France.
Cancers (Basel). 2021 Mar 13;13(6):1284. doi: 10.3390/cancers13061284.
In the PROSELICA phase III trial (NCT01308580), cabazitaxel 20 mg/m (CABA20) was non-inferior to cabazitaxel 25 mg/m (CABA25) in mCRPC patients previously treated with docetaxel (DOC). The present post hoc analysis evaluates how the type of progression at randomization affected outcomes.
Progression type at randomization was defined as follows: PSA progression only (PSA-p; no radiological progression (RADIO-p), no pain), RADIO-p (±PSA-p, no pain), or pain progression (PAIN-p, ±PSA-p, ±RADIO-p). Relationships between progression type and overall survival (OS), radiological progression-free survival (rPFS), and PSA response (confirmed PSA decrease ≥ 50%) were analyzed.
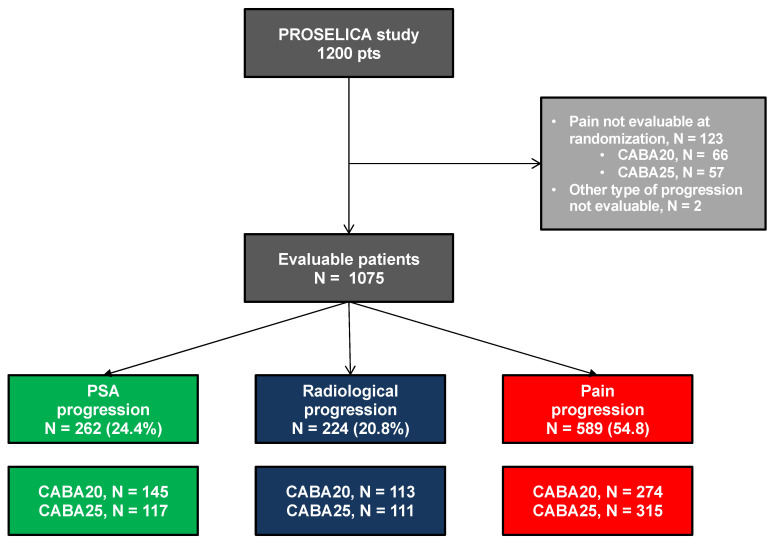
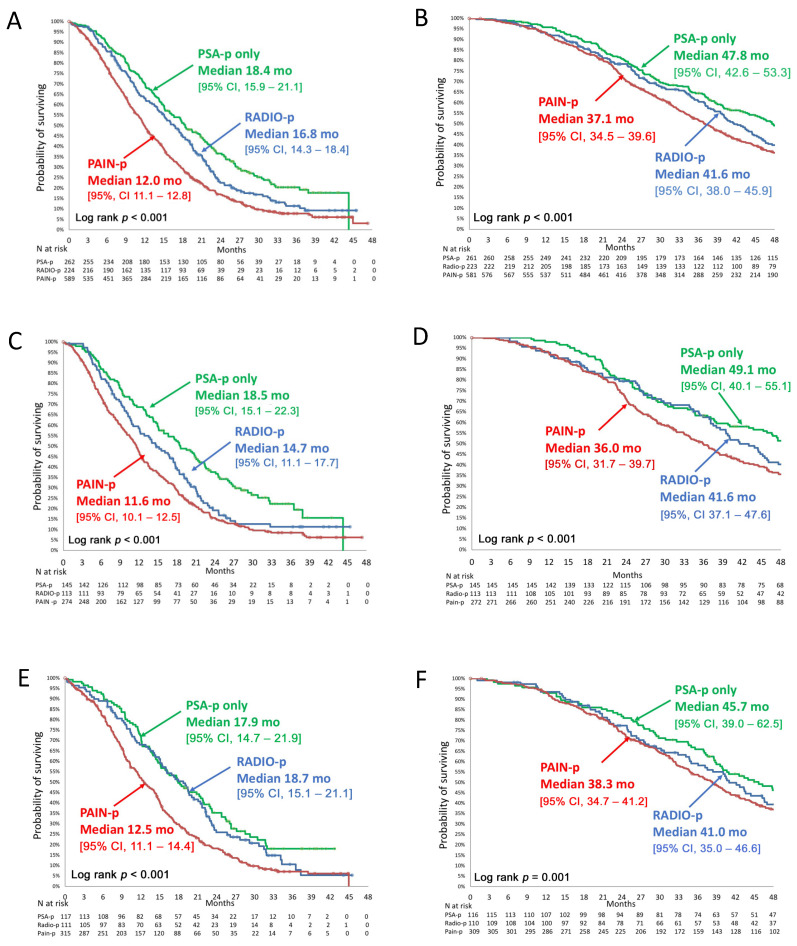
All randomized patients ( = 1200) had received prior DOC, and 25.7% had received prior abiraterone or enzalutamide. Progression type at randomization was evaluable in 1075 patients (PSA-p = 24.4%, RADIO-p = 20.8%, PAIN-p = 54.8%). Pain progression was associated with clinical and biological features of aggressive disease. Median OS from CABA initiation or date of mCRPC diagnosis, all arms combined, was shorter in the PAIN-p group than in the RADIO-p or the PSA-p groups (12.0 versus 16.8 and 18.4 months, respectively, < 0.001). In multivariate analysis, all arms combined, PAIN-p was an independent predictor of poor OS (HR = 1.44, < 0.001). PSA response, rPFS, and OS were numerically higher with CABA25 versus CABA20 in patients with PAIN-p.
This post hoc analysis of the PROSELICA phase III study shows that pain progression at initiation of CABA in mCRPC patients previously treated with DOC is associated with a poor prognosis. Disease progression should be carefully monitored, even in the absence of PSA rise.
在PROSELICA III期试验(NCT01308580)中,对于先前接受过多西他赛(DOC)治疗的转移性去势抵抗性前列腺癌(mCRPC)患者,20mg/m²的卡巴他赛(CABA20)不劣于25mg/m²的卡巴他赛(CABA25)。本事后分析评估了随机分组时的进展类型如何影响预后。
随机分组时的进展类型定义如下:仅前列腺特异抗原(PSA)进展(PSA-p;无影像学进展(RADIO-p),无疼痛)、影像学进展(RADIO-p(±PSA-p,无疼痛))或疼痛进展(PAIN-p,±PSA-p,±RADIO-p)。分析了进展类型与总生存期(OS)、无影像学进展生存期(rPFS)和PSA反应(确认PSA下降≥50%)之间的关系。
所有随机分组的患者(n = 1200)均接受过先前的DOC治疗,25.7%的患者接受过先前的阿比特龙或恩杂鲁胺治疗。1075例患者的随机分组时进展类型可评估(PSA-p = 24.4%,RADIO-p = 20.8%,PAIN-p = 54.8%)。疼痛进展与侵袭性疾病的临床和生物学特征相关。从开始使用CABA或mCRPC诊断日期起计算的中位OS,所有组合并,PAIN-p组短于RADIO-p组或PSA-p组(分别为12.0个月对16.8个月和18.4个月,P < 0.001)。在多变量分析中,所有组合并,PAIN-p是OS不良的独立预测因素(风险比 = 1.44,P < 0.001)。在PAIN-p患者中,与CABA20相比,CABA25的PSA反应、rPFS和OS在数值上更高。
PROSELICA III期研究的这项事后分析表明,先前接受DOC治疗的mCRPC患者开始使用CABA时的疼痛进展与预后不良相关。即使在PSA未升高的情况下,也应仔细监测疾病进展。