Martínez-Jiménez Mario, García-Gómez Pilar, Puig-Junoy Jaume
Division of Health Research, Faculty of Health & Medicine, Lancaster University, Lancaster LA1 4AT, UK.
Erasmus School of Economics, Erasmus University Rotterdam, P.O. Box 1738, 3000 DR Rotterdam, The Netherlands.
Int J Environ Res Public Health. 2021 Mar 4;18(5):2562. doi: 10.3390/ijerph18052562.
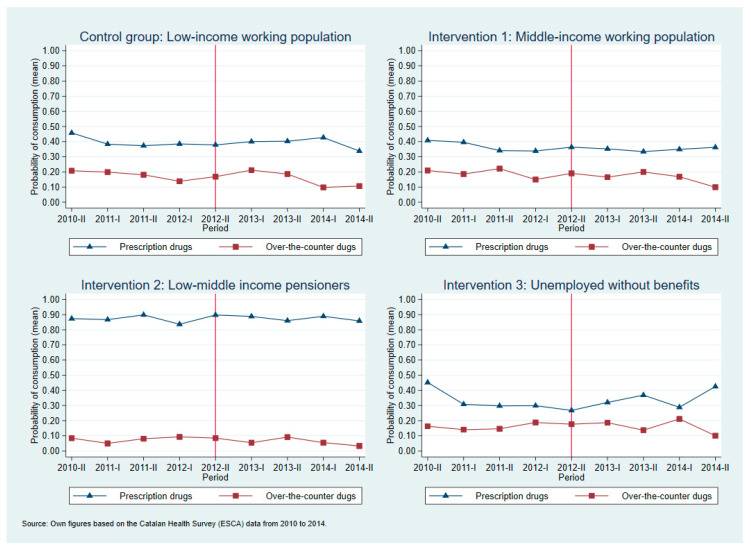
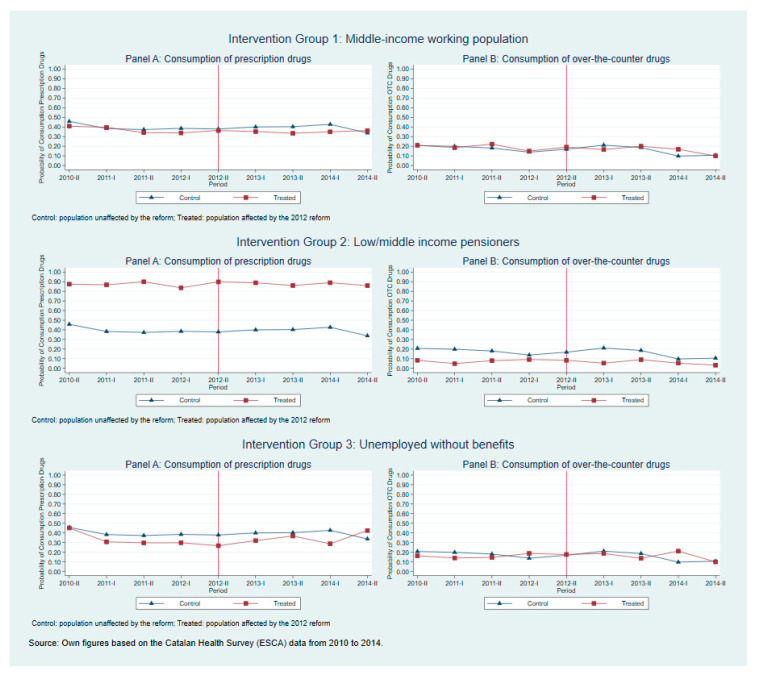
Many universal health care systems have increased the share of the price of medicines paid by the patient to reduce the cost pressure faced after the Great Recession. This paper assesses the impact of cost-sharing changes on the propensity to consume prescription and over-the-counter medicines in Catalonia, a Spanish autonomous community, affected by three new cost-sharing policies implemented in 2012. We applied a quasi-experimental difference-in-difference method using data from 2010 to 2014. These reforms were heterogeneous across different groups of individuals, so we define three intervention groups: (i) middle-income working population-co-insurance rate changed from 40% to 50%; (ii) low/middle-income pensioners-from free full coverage to 10% co-insurance rate; (iii) unemployed individuals without benefits-from 40% co-insurance rate to free full coverage. Our control group was the low-income working population whose co-insurance rate remained unchanged. We estimated the effects on the overall population as well as on the group with long-term care needs. We evaluated the effect of these changes on the propensity to consume prescription or over-the-counter medicines, and explored the heterogeneity effects across seven therapeutic groups of prescription medicines. Our findings showed that, on average, these changes did not significantly change the propensity to consume prescription or over-the-counter medicines. Nonetheless, we observed that the propensity to consume prescription medicines for mental disorders significantly increased among unemployed without benefits, while the consumption of prescribed mental disorders medicines for low/middle-income pensioners with long-term care needs decreased after becoming no longer free. We conclude that the propensity to consume medicines was not affected by the new cost-sharing policies, except for mental disorders. However, our results do not preclude potential changes in the quantity of medicines individuals consume.
许多全民医疗保健系统提高了患者支付药品价格的份额,以减轻大衰退后面临的成本压力。本文评估了成本分担变化对加泰罗尼亚(西班牙的一个自治区)处方药和非处方药消费倾向的影响,该地区在2012年实施了三项新的成本分担政策。我们采用了一种准实验性的差分法,使用了2010年至2014年的数据。这些改革在不同个体群体中存在差异,因此我们定义了三个干预组:(i)中等收入在职人群——共付率从40%变为50%;(ii)中低收入养老金领取者——从免费全额覆盖变为10%的共付率;(iii)无福利的失业人员——从40%的共付率变为免费全额覆盖。我们的对照组是共付率保持不变的低收入在职人群。我们估计了这些变化对总体人群以及有长期护理需求人群的影响。我们评估了这些变化对处方药或非处方药消费倾向的影响,并探讨了七个处方药治疗组之间的异质性影响。我们的研究结果表明,总体而言,这些变化并没有显著改变处方药或非处方药的消费倾向。尽管如此,我们观察到,无福利的失业人员中,精神障碍处方药的消费倾向显著增加,而对于有长期护理需求的中低收入养老金领取者,在不再免费后,精神障碍处方药的消费减少。我们得出结论,除了精神障碍药物外,药品消费倾向不受新成本分担政策的影响。然而,我们的结果并不排除个体药品消费量的潜在变化。