Department of Nephrology, Hypertension and Family Medicine, Medical University of Lodz, 90-549 Lodz, Poland.
Department of Urology, Institute of Medical Sciences, Medical College of Rzeszow University, 35-055 Rzeszow, Poland.
Toxins (Basel). 2021 Mar 31;13(4):252. doi: 10.3390/toxins13040252.
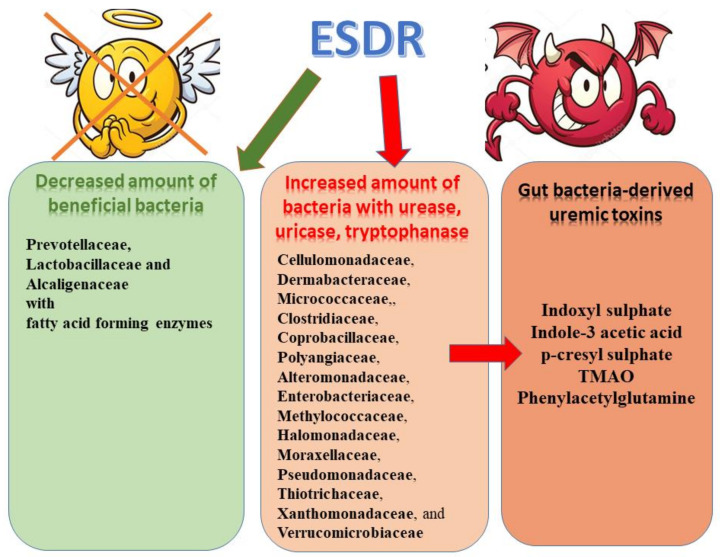
Numerous studies have indicated that the progression of chronic kidney disease (CKD) to end-stage renal disease (ESRD) is strictly associated with the accumulation of toxic metabolites in blood and other metabolic compartments. This accumulation was suggested to be related to enhanced generation of toxins from the dysbiotic microbiome accompanied by their reduced elimination by impaired kidneys. Intestinal microbiota play a key role in the accumulation of uremic toxins due to the fact that numerous uremic solutes are generated in the process of protein fermentation by colonic microbiota. Some disease states, including CKD, are associated with the presence of dysbiosis, which can be defined as an "imbalanced intestinal microbial community with quantitative and qualitative changes in the composition and metabolic activities of the gut microbiota". The results of studies have confirmed the altered composition and functions of gut microbial community in chronic kidney disease. In the course of CKD protein-bound uremic toxins, including indoxyl sulfate, p-cresyl glucuronide, p-cresyl sulfate and indole-3-acetic acid are progressively accumulated. The presence of chronic kidney disease may be accompanied by the development of intestinal inflammation and epithelial barrier impairment leading to hastened systemic translocation of bacterial-derived uremic toxins and consequent oxidative stress injury to the kidney, cardiovascular and endocrine systems. These findings offer new therapeutic possibilities for the management of uremia, inflammation and kidney disease progression and the prevention of adverse outcomes in CKD patients. It seems that dietary interventions comprising prebiotics, probiotics, and synbiotics could pose a promising strategy in the management of uremic toxins in CKD.
大量研究表明,慢性肾脏病(CKD)向终末期肾病(ESRD)的进展与血液和其他代谢隔室中有毒代谢物的积累密切相关。这种积累被认为与失调的微生物组产生的毒素增加有关,同时由于受损的肾脏,毒素的清除能力降低。由于大量尿毒症溶质是在结肠微生物群的蛋白质发酵过程中产生的,因此肠道微生物群在尿毒症毒素的积累中起着关键作用。一些疾病状态,包括 CKD,与失调有关,失调可以定义为“肠道微生物群落的不平衡,其组成和肠道微生物群的代谢活性发生了定量和定性变化”。研究结果证实了慢性肾脏病中肠道微生物群落的组成和功能发生了改变。在 CKD 过程中,蛋白质结合的尿毒症毒素(包括吲哚硫酸酯、对甲酚葡糖苷酸、对甲酚硫酸盐和吲哚-3-乙酸)逐渐积累。慢性肾脏病的存在可能伴随着肠道炎症和上皮屏障损伤的发展,导致细菌衍生的尿毒症毒素更快地全身转移,并对肾脏、心血管和内分泌系统造成氧化应激损伤。这些发现为尿毒症、炎症和肾脏疾病进展的管理以及 CKD 患者不良结局的预防提供了新的治疗可能性。似乎包含益生元、益生菌和合生菌的饮食干预可能是 CKD 中尿毒症毒素管理的一种有前途的策略。