Migliorini Filippo, Eschweiler Jörg, Maffulli Nicola, Schenker Hanno, Driessen Arne, Rath Björn, Tingart Markus
Department of Orthopedics and Trauma Surgery, University Clinic Aachen, RWTH Aachen University Clinic, 52064 Aachen, Germany.
School of Pharmacy and Bioengineering, Keele University School of Medicine, Staffordshire ST4 7QB, UK.
Life (Basel). 2021 Mar 16;11(3):244. doi: 10.3390/life11030244.
Many procedures are available to manage cartilage defects of the talus, including microfracturing (MFx) and Autologous Matrix Induced Chondrogenesis (AMIC). Whether AMIC or MFx are equivalent for borderline sized defects of the talar shoulder is unclear. Thus, the present study compared the efficacy of primary isolated AMIC versus MFx for borderline sized focal unipolar chondral defects of the talar shoulder at midterm follow-up.
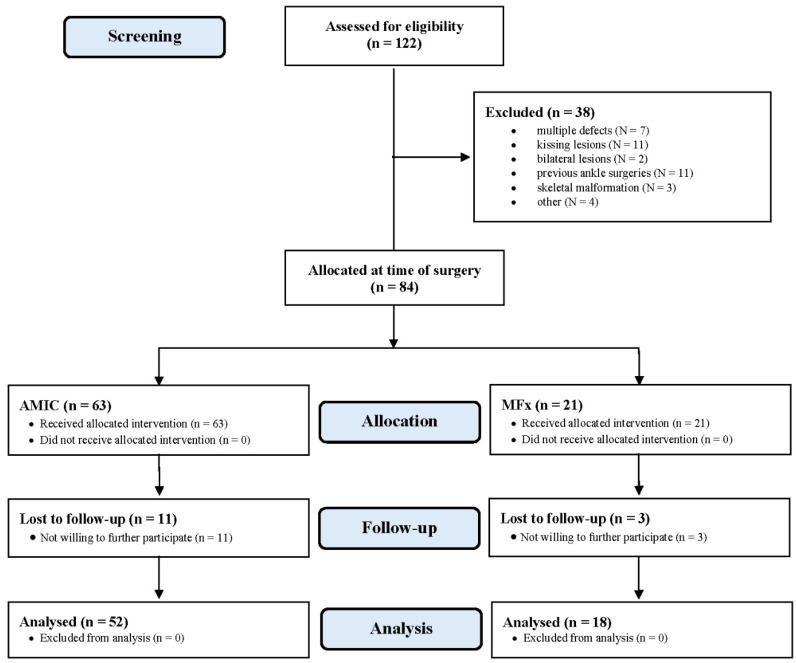
Patients undergoing primary isolated AMIC or MFx for focal unipolar borderline sized chondral defects of the talar shoulder were recruited prospectively. For those patients who underwent AMIC, a type I/III collagen resorbable membrane was used. The outcomes of interest were: Visual Analogic Scale (VAS), Tegner Activity Scale, American Orthopedic Foot and Ankle Score (AOFAS). The Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) was assessed by a blinded radiologist, who had not been involved in the clinical management of the patients. Data concerning complication rate and additional procedures were also collected.
The mean follow-up was 43.5 months. The mean age of the 70 patients at operation was 32.0 years, with a mean defect size of 2.7 cm. The mean length of hospitalization was shorter in the MFx cohort ( = 0.01). No difference was found between the two cohorts in terms of length of prior surgery symptoms and follow-up, mean age and BMI, sex and side, and defect size. At a mean follow-up of 43.5 months, the AOFAS ( = 0.03), VAS ( = 0.003), and Tegner ( = 0.01) scores were greater in the AMIC group. No difference was found in the MOCART score ( = 0.08). The AMIC group evidenced lower rates of reoperation ( = 0.008) and failure ( = 0.003).
At midterm follow-up, AMIC provides better results compared to MFx.
有多种方法可用于处理距骨软骨缺损,包括微骨折术(MFx)和自体基质诱导软骨形成术(AMIC)。对于距骨肩部临界尺寸的缺损,AMIC和MFx是否等效尚不清楚。因此,本研究比较了初次单独使用AMIC与MFx治疗距骨肩部临界尺寸的局灶性单极软骨缺损在中期随访时的疗效。
前瞻性招募因距骨肩部局灶性单极临界尺寸软骨缺损而接受初次单独AMIC或MFx治疗的患者。对于接受AMIC治疗的患者,使用I/III型胶原可吸收膜。感兴趣的结果指标包括:视觉模拟评分量表(VAS)、特格纳活动量表、美国矫形足踝评分(AOFAS)。由一名未参与患者临床管理的盲法放射科医生评估软骨修复组织的磁共振观察(MOCART)。还收集了有关并发症发生率和额外手术的数据。
平均随访时间为43.5个月。70例患者手术时的平均年龄为32.0岁,平均缺损大小为2.7厘米。MFx队列的平均住院时间较短(P = 0.01)。两组在既往手术症状持续时间、随访时间、平均年龄和体重指数、性别和患侧以及缺损大小方面均未发现差异。在平均随访43.5个月时,AMIC组的AOFAS评分(P = 0.03)、VAS评分(P = 0.003)和特格纳评分(P = 0.01)更高。MOCART评分未发现差异(P = 0.08)。AMIC组的再次手术率(P = 0.008)和失败率(P = 0.003)较低。
在中期随访时,与MFx相比,AMIC的效果更好。