Springer Jan, Held Jürgen, Mengoli Carlo, Schlegel Paul Gerhardt, Gamon Florian, Träger Johannes, Kurzai Oliver, Einsele Hermann, Loeffler Juergen, Eyrich Matthias
Department for Internal Medicine II, University Hospital of Würzburg, 97080 Würzburg, Germany.
Mikrobiologisches Institut-Klinische Mikrobiologie, Immunologie und Hygiene, Universitätsklinikum Erlangen und Friedrich-Alexander-Universität (FAU) Erlangen-Nürnberg, 91054 Erlangen, Germany.
J Fungi (Basel). 2021 Mar 22;7(3):238. doi: 10.3390/jof7030238.
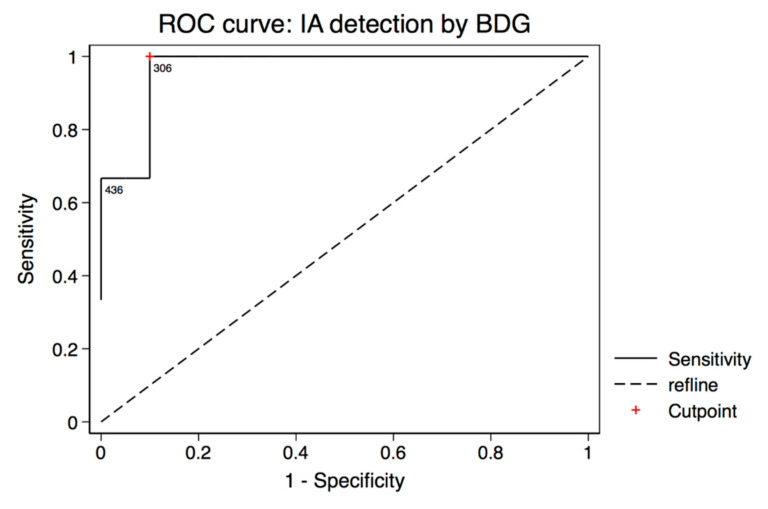
Data on biomarker-assisted diagnosis of invasive aspergillosis (IA) in pediatric patients is scarce. Therefore, we conducted a cohort study over two years including 404 serum specimens of 26 pediatric patients after allogeneic hematopoietic stem cell transplantation (alloSCT). Sera were tested prospectively twice weekly for -specific DNA, galactomannan (GM), and retrospectively for (1→3)-β-D-glucan (BDG). Three probable IA and two possible invasive fungal disease (IFD) cases were identified using the European Organization for Research and Treatment of Cancer and the Mycoses Study Group (EORTC/MSGERC) 2019 consensus definitions. Sensitivity and specificity for diagnosis of probable IA and possible IFD was 80% (95% confidential interval (CI): 28-99%) and 55% (95% CI: 32-77%) for BDG, 40% (95% CI: 5-85%) and 100% (95% CI: 83-100%) for GM, and 60% (95% CI: 15-95%) and 95% (95% CI: 75-100%) for specific real-time PCR. However, sensitivities have to be interpreted with great caution due to the limited number of IA cases. Interestingly, the low specificity of BDG was largely caused by false-positive BDG results that clustered around the date of alloSCT. The following strategies were able to increase BDG specificity: two consecutive positive BDG tests for diagnosis (specificity 80% (95% CI: 56-94%)); using an optimized cutoff value of 306 pg/mL (specificity 90% (95% CI: 68-99%)) and testing BDG only after the acute posttransplant phase. In summary, BDG can help to diagnose IA in pediatric alloSCT recipients. However, due to the poor specificity either an increased cutoff value should be utilized or BDG results should be confirmed by an alternative assay.
关于生物标志物辅助诊断儿童侵袭性曲霉病(IA)的数据很少。因此,我们进行了一项为期两年的队列研究,纳入了26例接受异基因造血干细胞移植(alloSCT)的儿科患者的404份血清标本。前瞻性地每周两次检测血清中的曲霉特异性DNA、半乳甘露聚糖(GM),并回顾性检测(1→3)-β-D-葡聚糖(BDG)。采用欧洲癌症研究与治疗组织和真菌病研究组(EORTC/MSGERC)2019年共识定义,确定了3例可能的IA和2例可能的侵袭性真菌病(IFD)病例。BDG诊断可能的IA和可能的IFD的敏感性和特异性分别为80%(95%置信区间(CI):28-99%)和55%(95%CI:32-77%),GM分别为40%(95%CI:5-85%)和100%(95%CI:83-100%),曲霉特异性实时PCR分别为60%(95%CI:15-95%)和95%(95%CI:75-100%)。然而,由于IA病例数量有限,对敏感性的解释必须非常谨慎。有趣的是,BDG的低特异性很大程度上是由alloSCT日期前后聚集的BDG假阳性结果引起的。以下策略能够提高BDG的特异性:连续两次BDG检测阳性用于诊断(特异性80%(95%CI:56-94%));使用306 pg/mL的优化临界值(特异性90%(95%CI:68-99%)),并且仅在移植后急性期过后检测BDG。总之,BDG有助于诊断儿科alloSCT受者的IA。然而,由于特异性较差,要么应采用更高的临界值,要么应通过另一种检测方法确认BDG结果。