Department of Cardiology Oslo University Hospital, Rikshospitalet Norway.
Faculty of Medicine Institute of Clinical MedicineUniversity of Oslo Norway.
J Am Heart Assoc. 2021 Apr 20;10(8):e018680. doi: 10.1161/JAHA.120.018680. Epub 2021 Apr 6.
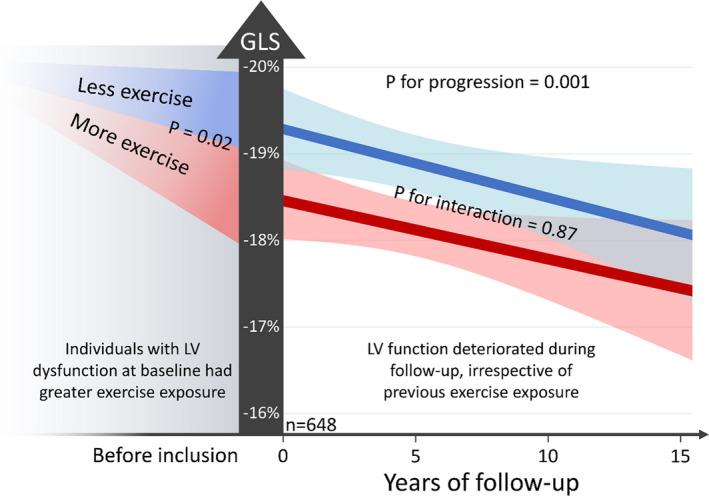
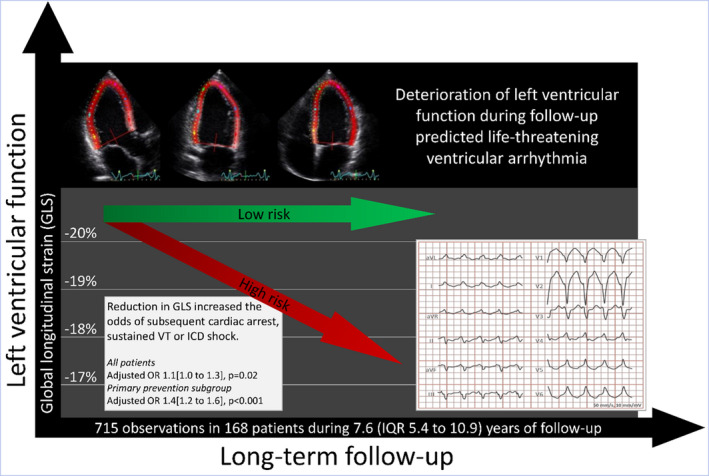
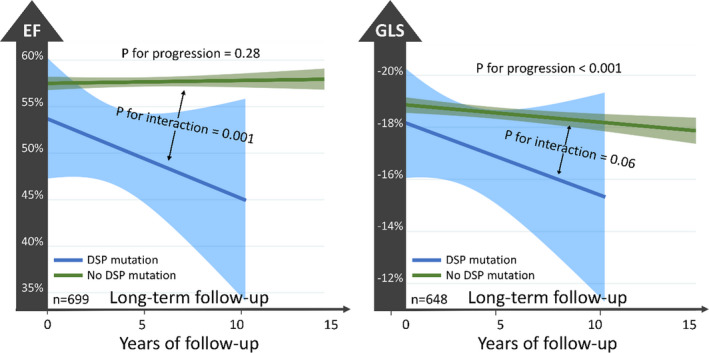
Background Arrhythmogenic cardiomyopathy (AC) is characterized by biventricular dysfunction, exercise intolerance, and high risk of ventricular tachyarrhythmias and sudden death. Predisposing factors for left ventricular (LV) disease manifestation and its prognostic implication in AC are poorly described. We aimed to assess the associations of exercise exposure and genotype with LV dysfunction in AC, and to explore the impact of LV disease progression on adverse arrhythmic outcome. Methods and Results We included 168 patients with AC (50% probands, 45% women, 40±16 years old) with 715 echocardiographic exams (4.1±1.7 exams/patient, follow-up 7.6 [interquartile range (IQR), 5.4-10.9] years) and complete exercise and genetic data in a longitudinal study. LV function by global longitudinal strain was -18.8% [IQR, -19.2% to -18.3%] at presentation and was worse in patients with greater exercise exposure (global longitudinal strain worsening, 0.09% [IQR, 0.01%-0.17%] per 5 MET-hours/week, =0.02). LV function by global longitudinal strain worsened, with 0.08% [IQR, 0.05%-0.12%] per year; (<0.001), and progression was most evident in patients with desmoplakin genotype ( for interaction <0.001). Deterioration of LV function predicted incident ventricular tachyarrhythmia (aborted cardiac arrest, sustained ventricular tachycardia, or implantable cardioverter defibrillator shock) (adjusted odds ratio, 1.1 [IQR, 1.0-1.3] per 1% worsening by global longitudinal strain; =0.02, adjusted for time and previous arrhythmic events). Conclusions Greater exercise exposure was associated with worse LV function at first visit of patients with AC but did not significantly affect the rate of LV progression during follow-up. Progression of LV dysfunction was most pronounced in patients with desmoplakin genotypes. Deterioration of LV function during follow-up predicted subsequent ventricular tachyarrhythmia and should be considered in risk stratification.
背景 致心律失常性右室心肌病(AC)的特征为双心室功能障碍、运动不耐受,以及发生室性心动过速和心源性猝死的风险较高。左心室(LV)疾病表现的诱发因素及其对 AC 的预后意义描述甚少。我们旨在评估运动暴露和基因型与 AC 中 LV 功能障碍的相关性,并探讨 LV 疾病进展对不良心律失常结局的影响。
方法和结果 我们纳入了 168 例 AC 患者(50%先证者,45%为女性,40±16 岁),这些患者在一项纵向研究中接受了 715 次超声心动图检查(4.1±1.7 次/患者,随访 7.6 [四分位距(IQR),5.4-10.9] 年),并完成了运动和基因数据的采集。在初次就诊时,通过整体纵向应变评估的 LV 功能为-18.8%[IQR,-19.2%至-18.3%],而运动暴露较多的患者的 LV 功能更差(整体纵向应变恶化,每 5 梅脱小时/周增加 0.09%[IQR,0.01%-0.17%],=0.02)。LV 功能以整体纵向应变表示,每年恶化 0.08%[IQR,0.05%-0.12%];(<0.001),并且在桥粒芯糖蛋白基因型的患者中进展最为明显(=0.001)。LV 功能恶化预测发生室性心律失常(心源性猝死、持续性室性心动过速或植入式心脏复律除颤器电击)(调整后比值比,每 1%整体纵向应变恶化 1.1[IQR,1.0-1.3];=0.02,调整时间和之前的心律失常事件)。
结论 在 AC 患者初次就诊时,更多的运动暴露与 LV 功能较差相关,但在随访期间对 LV 进展的速度没有显著影响。桥粒芯糖蛋白基因型患者的 LV 功能障碍进展最为明显。随访期间 LV 功能恶化预测随后发生室性心律失常,应在危险分层中加以考虑。