Department of Family Medicine.
OHSU-PSU School of Public Health, OHSU.
Med Care. 2021 May 1;59(5):402-409. doi: 10.1097/MLR.0000000000001527.
Our understanding of how multimorbidity progresses and changes is nascent.
Assess multimorbidity changes among racially/ethnically diverse middle-aged and older adults.
DESIGN, SETTING, AND PARTICIPANTS: Prospective cohort study using latent class analysis to identify multimorbidity combinations over 16 years, and multinomial logistic models to assess change relative to baseline class membership. Health and Retirement Study respondents (age 51 y and above) in 1998 and followed through 2014 (N=17,297).
Multimorbidity latent classes of: hypertension, heart disease, lung disease, diabetes, cancer, arthritis, stroke, high depressive symptoms.
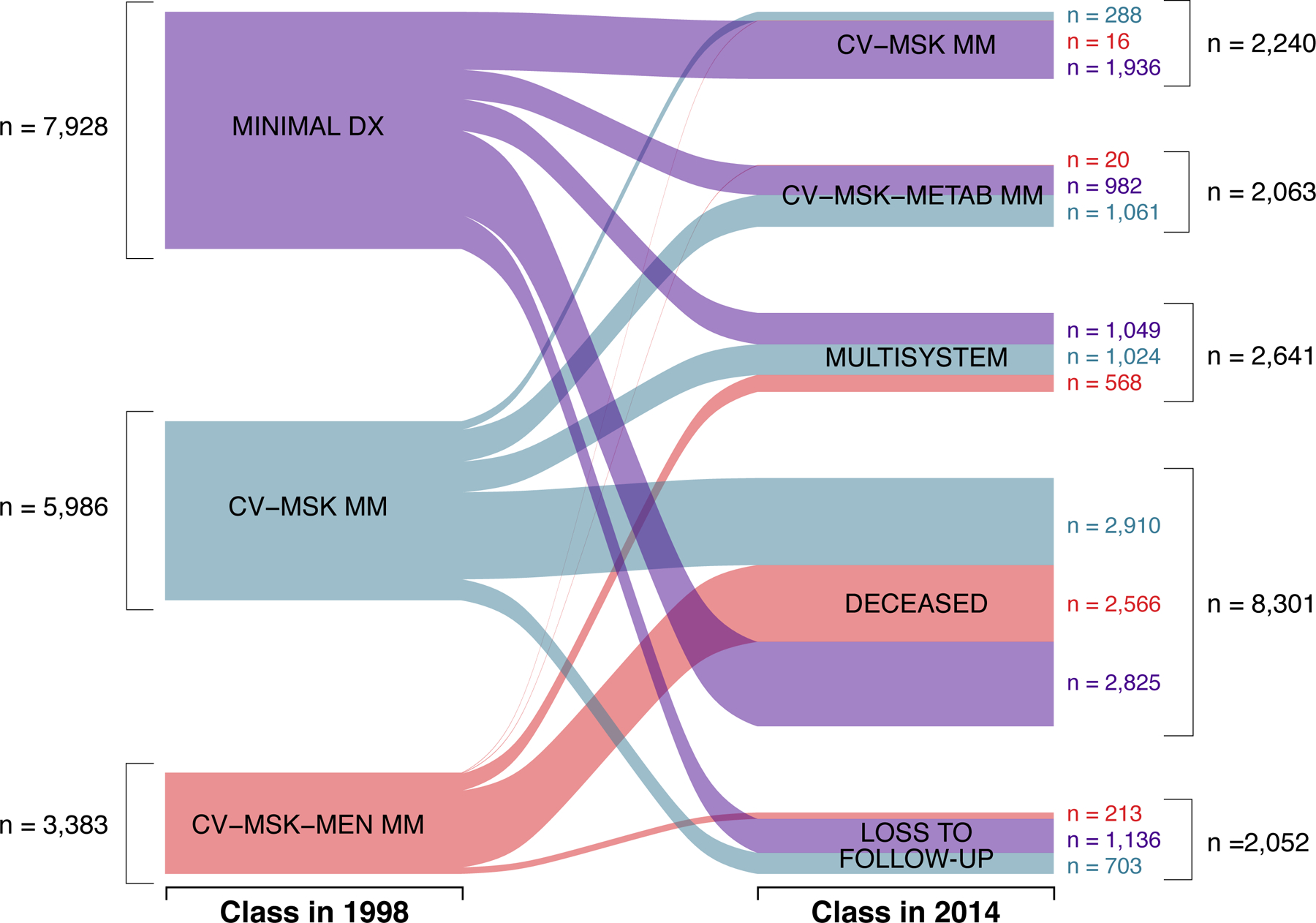
Three latent classes were identified in 1998: minimal disease (45.8% of participants), cardiovascular-musculoskeletal (34.6%), cardiovascular-musculoskeletal-mental (19.6%); and 3 in 2014: cardiovascular-musculoskeletal (13%), cardiovascular-musculoskeletal-metabolic (12%), multisystem multimorbidity (15%). Remaining participants were deceased (48%) or lost to follow-up (12%) by 2014. Compared with minimal disease, individuals in cardiovascular-musculoskeletal in 1998 were more likely to be in multisystem multimorbidity in 2014 [odds ratio (OR)=1.78, P<0.001], and individuals in cardiovascular-musculoskeletal-mental in 1998 were more likely to be deceased (OR=2.45, P<0.001) or lost to follow-up (OR=3.08, P<0.001). Hispanic and Black Americans were more likely than White Americans to be in multisystem multimorbidity in 2014 (OR=1.67, P=0.042; OR=2.60, P<0.001, respectively). Black compared with White Americans were more likely to be deceased (OR=1.62, P=0.01) or lost to follow-up (OR=2.11, P<0.001) by 2014.
Racial/ethnic older adults are more likely to accumulate morbidity and die compared with White peers, and should be the focus of targeted and enhanced efforts to prevent and/or delay progression to more complex multimorbidity patterns.
我们对多种疾病的发展和变化的理解还处于起步阶段。
评估不同种族/族裔的中年和老年人的多种疾病变化情况。
设计、地点和参与者:使用潜在类别分析在 16 年内识别多种疾病的组合,并使用多项逻辑回归模型评估与基线类别成员关系的变化。1998 年参加健康与退休研究(年龄在 51 岁及以上)的受访者,并于 2014 年进行随访(N=17297)。
高血压、心脏病、肺病、糖尿病、癌症、关节炎、中风、高抑郁症状的多种疾病潜在类别。
1998 年确定了三个潜在类别:轻微疾病(45.8%的参与者)、心血管-肌肉骨骼(34.6%)、心血管-肌肉骨骼-心理(19.6%);2014 年有三个:心血管-肌肉骨骼(13%)、心血管-肌肉骨骼-代谢(12%)、多系统多种疾病(15%)。其余参与者在 2014 年已死亡(48%)或失访(12%)。与轻微疾病相比,1998 年患有心血管-肌肉骨骼疾病的个体在 2014 年更有可能患有多系统多种疾病[优势比(OR)=1.78,P<0.001],而 1998 年患有心血管-肌肉骨骼-心理疾病的个体更有可能死亡(OR=2.45,P<0.001)或失访(OR=3.08,P<0.001)。西班牙裔和非裔美国人比白人更有可能在 2014 年患有多系统多种疾病(OR=1.67,P=0.042;OR=2.60,P<0.001)。与白人相比,黑人更有可能在 2014 年死亡(OR=1.62,P=0.01)或失访(OR=2.11,P<0.001)。
与白人同龄人相比,不同种族/族裔的老年人群更有可能患上多种疾病并死亡,应成为有针对性和强化努力的重点,以预防和/或延迟向更复杂的多种疾病模式发展。