Gastrointestinal Oncology Unit, Medical Clinic 1, Goethe University Hospital Frankfurt, Theodor-Stern-Kai 7, 60590, Frankfurt, Germany.
Ipsen Pharma, Boulogne-Billancourt, France.
Adv Ther. 2021 May;38(5):2472-2490. doi: 10.1007/s12325-021-01700-2. Epub 2021 Apr 6.
Cabozantinib and ramucirumab are approved for the treatment of adults with hepatocellular carcinoma (HCC) following prior sorafenib treatment; ramucirumab is restricted to use in patients with serum alpha-fetoprotein (AFP) ≥ 400 ng/mL. This matching-adjusted indirect comparison evaluated the efficacy and safety of both drugs after sorafenib in patients with HCC and AFP ≥ 400 ng/mL.
Individual patient data (IPD) from the CELESTIAL trial (cabozantinib) and population-level data from the REACH-2 trial (ramucirumab) were used. To align with REACH-2, the CELESTIAL population was limited to patients who received first-line sorafenib only and had baseline serum AFP ≥ 400 ng/mL. The IPD from CELESTIAL were weighted to balance the distribution of 11 effect-modifying baseline characteristics with those of REACH-2. Overall survival (OS; primary endpoint) and progression-free survival (PFS) were compared for the CELESTIAL (matching-adjusted) and REACH-2 populations using weighted Kaplan-Meier (KM) curves and parametric (OS, Weibull; PFS, log-logistic) modeling. Rates of treatment-related adverse events (TRAEs) and TRAE-related discontinuations were also compared.
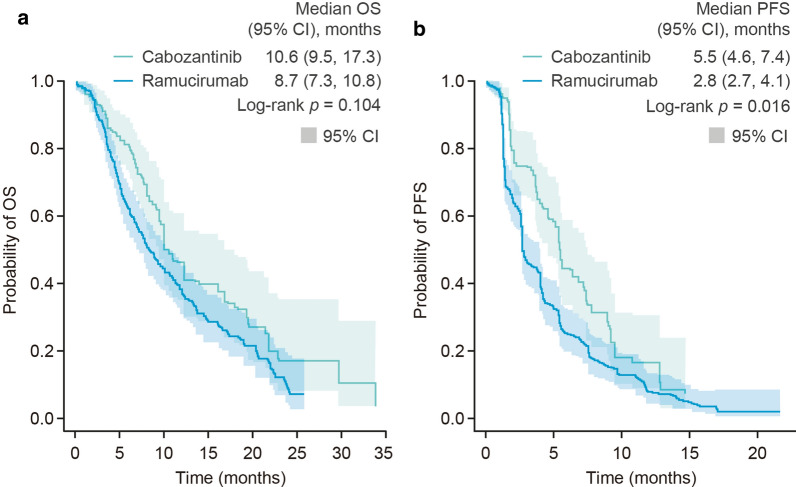
After matching and weighting, baseline characteristics were balanced between populations (REACH-2, N = 292; CELESTIAL, effective sample size = 105). Weighted KM estimates for OS (median [95% CI]) were not significantly different between cabozantinib and ramucirumab (10.6 [9.5-17.3] months versus 8.7 [7.3-10.8] months; p = 0.104), but PFS was significantly longer for cabozantinib than for ramucirumab (5.5 [4.6-7.4] months versus 2.8 [2.7-4.1] months; p = 0.016). Parametric modeling results were consistent with the weighted KM analysis. Rates of some grade 3 or 4 TRAEs were lower with ramucirumab than with cabozantinib; however, TRAE-related discontinuation rates were similar (p = 0.271).
In this MAIC, cabozantinib significantly prolonged median PFS compared with ramucirumab after prior sorafenib treatment in patients with HCC and AFP ≥ 400 ng/mL; rates of some grade 3 or 4 TRAEs were lower with ramucirumab than cabozantinib but related discontinuation rates were not significantly different between treatments.
Clinical trials.gov identifiers: CELESTIAL trial (NCT01908426) and REACH-2 trial (NCT02435433). These slides can be retrieved under Electronic Supplementary Material.
卡博替尼和雷莫芦单抗已被批准用于索拉非尼治疗后的肝癌(HCC)成人患者;雷莫芦单抗仅限制用于血清甲胎蛋白(AFP)≥400ng/mL 的患者。这项匹配调整的间接比较评估了卡博替尼和雷莫芦单抗在 AFP≥400ng/mL 的 HCC 患者中的疗效和安全性。
CELESTIAL 试验的个体患者数据(IPD)(卡博替尼)和 REACH-2 试验的人群水平数据(雷莫芦单抗)被使用。为了与 REACH-2 保持一致,CELESTIAL 人群仅限于仅接受一线索拉非尼治疗且基线血清 AFP≥400ng/mL 的患者。来自 CELESTIAL 的 IPD 经过加权处理,以平衡 11 个影响疗效的基线特征的分布与 REACH-2 的分布。使用加权 Kaplan-Meier(KM)曲线和参数(OS,Weibull;PFS,log-logistic)模型比较 CELESTIAL(匹配调整)和 REACH-2 人群的总生存期(OS;主要终点)和无进展生存期(PFS)。还比较了治疗相关不良事件(TRAEs)和 TRAE 相关停药率。
匹配和加权后,人群之间的基线特征得到了平衡(REACH-2,N=292;CELESTIAL,有效样本量=105)。OS 的加权 KM 估计值(中位数[95%CI])在卡博替尼和雷莫芦单抗之间没有显著差异(10.6[9.5-17.3]个月与 8.7[7.3-10.8]个月;p=0.104),但卡博替尼的 PFS 明显长于雷莫芦单抗(5.5[4.6-7.4]个月与 2.8[2.7-4.1]个月;p=0.016)。参数建模结果与加权 KM 分析一致。一些 3 级或 4 级 TRAEs 的发生率雷莫芦单抗低于卡博替尼,但 TRAE 相关停药率相似(p=0.271)。
在这项 MAIC 中,卡博替尼在 AFP≥400ng/mL 的 HCC 患者中,在索拉非尼治疗后,与雷莫芦单抗相比,显著延长了中位 PFS;一些 3 级或 4 级 TRAEs 的发生率雷莫芦单抗低于卡博替尼,但治疗相关停药率无显著差异。
临床试验.gov 标识符:CELESTIAL 试验(NCT01908426)和 REACH-2 试验(NCT02435433)。这些幻灯片可在电子补充材料中检索。