Department of Obstetrics and Gynecology, University Hospital, LMU Munich, Munich, Germany.
Munich Cancer Registry, Bavarian Cancer Registry - Regional Centre Munich (LGL) at the University Hospital of Munich, Institute for Medical Information Processing, Biometry and Epidemiology, LMU Munich, Munich, Germany.
J Gynecol Oncol. 2021 May;32(3):e37. doi: 10.3802/jgo.2021.32.e37.
Patients with platinum-resistant ovarian cancer (PROC) have a high need for reliable prognostic markers. Since significance of primary platinum resistance (PPR) versus secondary platinum resistance (SPR) was identified for patients receiving anti-angiogenic therapy, it has not been confirmed for chemotherapy only.
PROC patients from 3 prospective trials of the NOGGO study group (TOWER, NOGGO-Treosulfan, and TRIAS) were included in this meta-analysis. Exploratory Cox and logistic regression analyses were performed to correlate progression-free survival (PFS) and overall survival (OS) with the timing when platinum resistance developed.
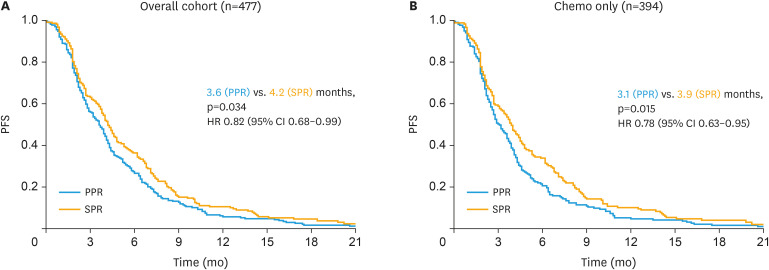
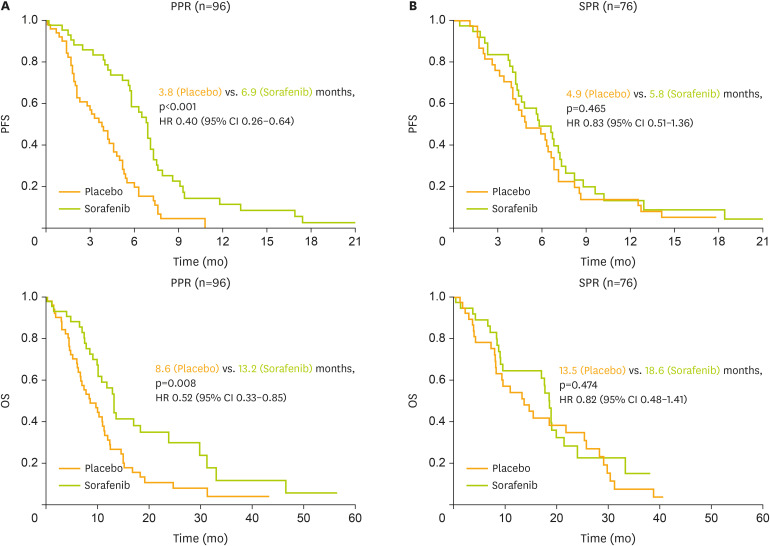
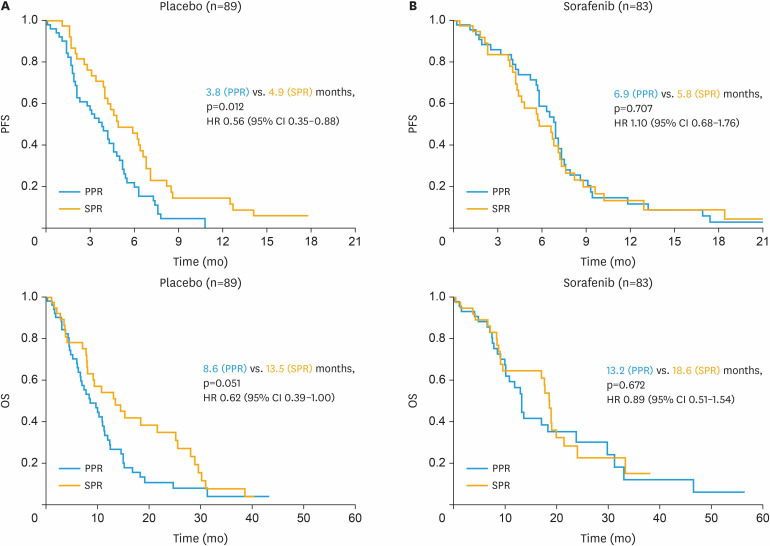
Of 477 patients, 264 (55.3%) were classified as PPR, compared to 213 (44.7%) with SPR. For patients receiving chemotherapy only, SPR was associated with a significantly longer median PFS of 3.9 compared to 3.1 months for PPR (hazard ratio [HR]=0.78; p=0.015). SPR versus PPR was confirmed to be an independent prognostic factor for better PFS in multivariate analysis (HR=0.74; p=0.029). Benefit from adding sorafenib to chemotherapy was mainly seen in PPR (HR=0.40; p<0.001) compared to SPR patients (HR=0.83; p=0.465).
Prognostic significance of SPR versus PPR could be elucidated for patients receiving chemotherapy only. In contrast to bevacizumab, the multi-kinase inhibitor sorafenib exhibits profound therapeutic efficacy in PPR patients indicating potential to overcome this negative prognostic impact.
铂耐药卵巢癌(PROC)患者对可靠的预后标志物有很高的需求。由于原发性铂耐药(PPR)与继发性铂耐药(SPR)对接受抗血管生成治疗的患者具有重要意义,但其对于仅接受化疗的患者尚未得到证实。
本研究纳入了来自 NOGGO 研究组的 3 项前瞻性试验(TOWER、NOGGO-Treosulfan 和 TRIAS)的 PROC 患者。进行探索性 Cox 和逻辑回归分析,以将无进展生存期(PFS)和总生存期(OS)与铂耐药发生的时间相关联。
在 477 名患者中,264 名(55.3%)被归类为 PPR,而 213 名(44.7%)为 SPR。对于仅接受化疗的患者,SPR 与明显更长的中位 PFS 相关,为 3.9 个月,而 PPR 为 3.1 个月(风险比[HR]=0.78;p=0.015)。SPR 相对于 PPR 在多变量分析中被证实是更好的 PFS 的独立预后因素(HR=0.74;p=0.029)。与 SPR 患者相比(HR=0.83;p=0.465),索拉非尼添加到化疗中可使 PPR 患者获益(HR=0.40;p<0.001)。
对于仅接受化疗的患者,SPR 相对于 PPR 的预后意义可以阐明。与贝伐单抗不同,多激酶抑制剂索拉非尼在 PPR 患者中显示出显著的治疗效果,表明有可能克服这种负面预后影响。