Rossi Marco, Gay Lorenzo, Conti Nibali Marco, Sciortino Tommaso, Ambrogi Federico, Leonetti Antonella, Puglisi Guglielmo, Howells Henrietta, Zito Paola, Villa Federico, Ciroi Gjulio, Riva Marco, Bello Lorenzo
Neurosurgical Oncological Unit, Department of Oncology and Hemato-Oncology, Università Degli Studi di Milano, Milano, Italy.
Laboratory of Medical Statistics, Biometry, and Epidemiology "G.A. Maccararo," Department of Clinical Sciences and Community Health, Università degli Studi di Milano, Milano, Italy.
Front Oncol. 2021 Mar 22;11:629166. doi: 10.3389/fonc.2021.629166. eCollection 2021.
Giant insular tumors are commonly not amenable to complete resection and are associated with a high postoperative morbidity rate. Transcortical approach and brain mapping techniques allow to identify peri-insular functional networks and, with neurophysiological monitoring, to reduce vascular-associated insults. Cognitive functions to be mapped are still under debate, and the analysis of the functional risk of surgery is currently limited to neurological examination. This work aimed to investigate the neurosurgical outcome (extent of resection, EOR) and functional impact of giant insular gliomas resection, focusing on neuropsychological and Quality of Life (QoL) outcomes.
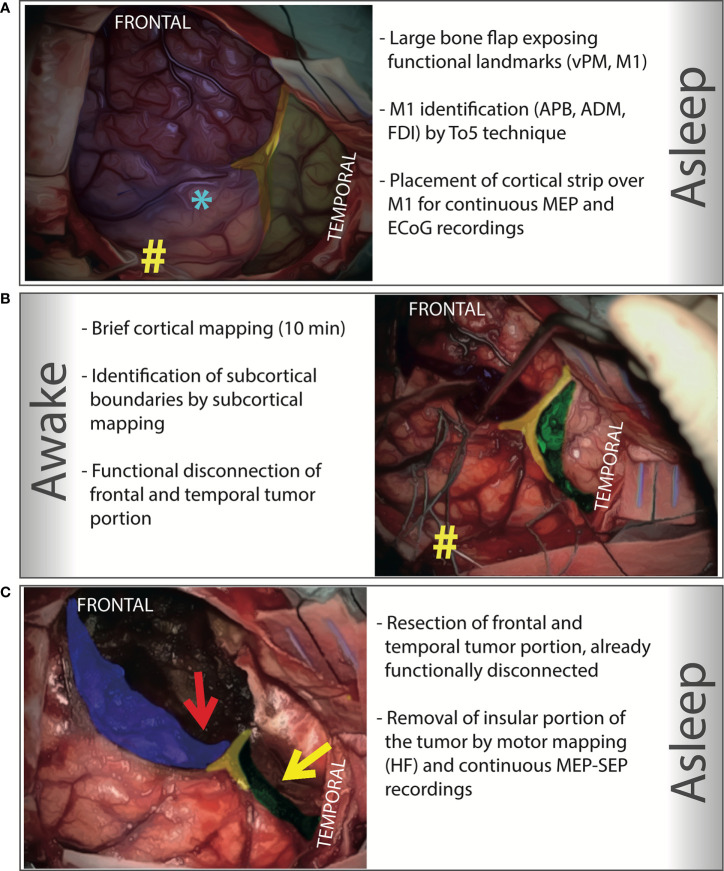
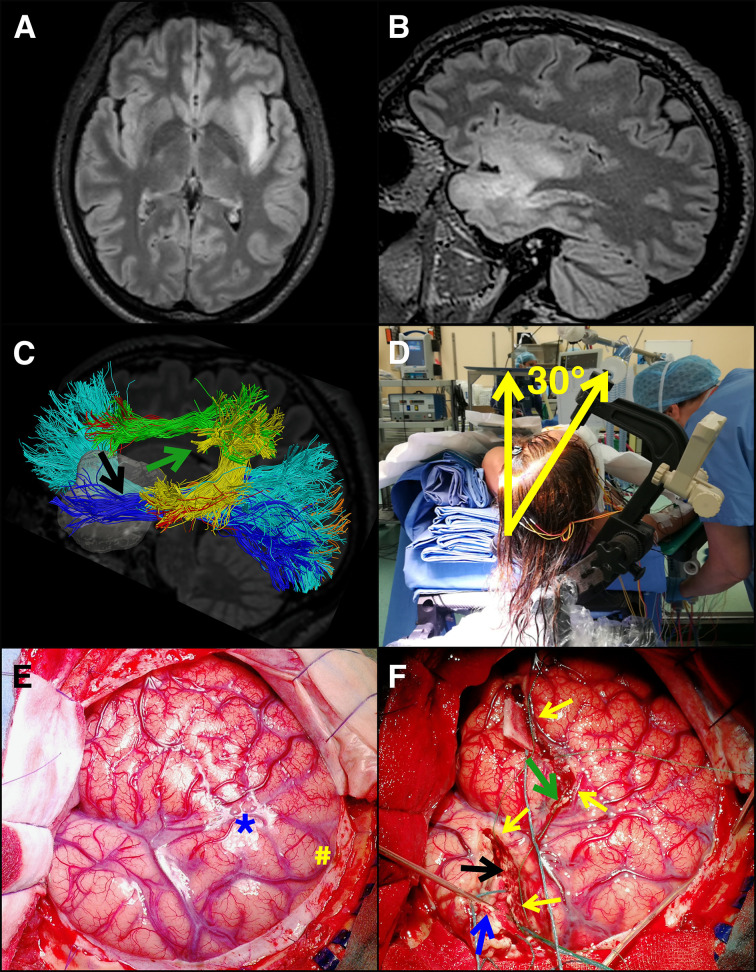
In our retrospective analysis, we included all patients admitted in a five-year period with a radiological diagnosis of giant insular glioma. A transcortical approach was adopted in all cases. Resections were pursued up to functional boundaries defined intraoperatively by brain mapping techniques. We examined clinical, radiological, and intra-operative factors possibly affecting EOR and postoperative neurological, neuropsychological, and Quality of Life (QoL) outcomes.
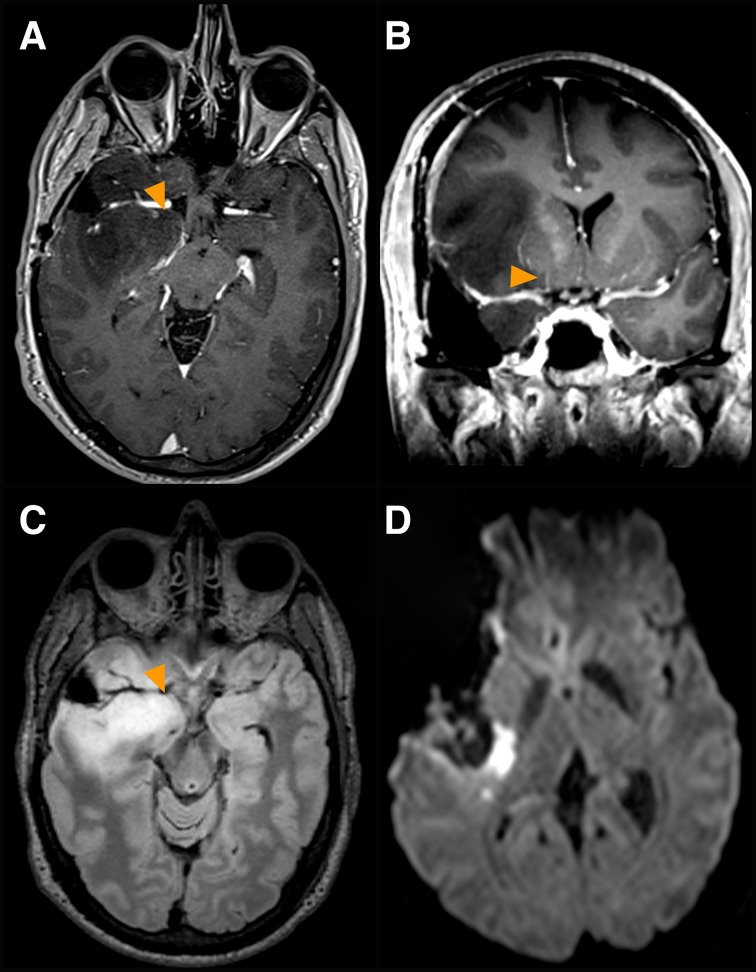
We finally enrolled 95 patients in the analysis. Mean EOR was 92.3%. A Gross Total Resection (GTR) was obtained in 70 cases (73.7%). Five patients reported permanent morbidity (aphasia in 3, 3.2%, and superior quadrantanopia in 2, 2.1%). Suboptimal EOR associated with poor seizures control postoperatively. Extensive intraoperative mapping (inclusive of cognitive, visual, and haptic functions) decreased long-term neurological, neuropsychological, and QoL morbidity and increased EOR. Tumor infiltration of deep perforators (vessels arising either medial to lenticulostriate arteries through the anterior perforated substance or from the anterior choroidal artery) associated with a higher chance of postoperative ischemia in consonant areas, with the persistence of new-onset motor deficits 1-month post-op, and with minor EOR. Ischemic insults in eloquent sites represented the leading factor for long-term neurological and neuropsychological morbidity.
In giant insular gliomas, the use of a transcortical approach with extensive brain mapping under awake anesthesia ensures broad insular exposure and extension of the surgical resection preserving patients' functional integrity. The relation between tumor mass and deep perforators predicts perioperative ischemic insults, the most relevant risk factor for long-term and permanent postoperative morbidity.
巨大岛叶肿瘤通常难以完全切除,且术后发病率较高。经皮质入路和脑图谱技术有助于识别岛叶周围的功能网络,并通过神经生理监测减少与血管相关的损伤。有待绘制图谱的认知功能仍存在争议,目前手术功能风险分析仅限于神经学检查。本研究旨在探讨巨大岛叶胶质瘤切除的神经外科手术结果(切除范围,EOR)及其功能影响,重点关注神经心理学和生活质量(QoL)结果。
在我们的回顾性分析中,纳入了五年内所有经影像学诊断为巨大岛叶胶质瘤的患者。所有病例均采用经皮质入路。根据脑图谱技术术中确定的功能边界进行切除。我们检查了可能影响EOR以及术后神经、神经心理学和生活质量(QoL)结果的临床、影像学和术中因素。
我们最终纳入95例患者进行分析。平均EOR为92.3%。70例(73.7%)实现了全切除(GTR)。5例患者出现永久性并发症(3例失语,3.2%;2例上象限盲,2.1%)。EOR欠佳与术后癫痫控制不佳相关。广泛的术中图谱绘制(包括认知、视觉和触觉功能)可降低长期神经、神经心理学和QoL并发症的发生率,并提高EOR。深部穿支血管(通过前穿质在豆纹动脉内侧发出的血管或来自脉络膜前动脉的血管)受肿瘤浸润,与相应区域术后缺血几率增加、术后1个月新发运动功能缺损持续存在以及EOR较小相关。明确部位的缺血性损伤是长期神经和神经心理学并发症的主要因素。
对于巨大岛叶胶质瘤,在清醒麻醉下采用经皮质入路并进行广泛的脑图谱绘制,可确保广泛暴露岛叶并扩大手术切除范围,同时保留患者的功能完整性。肿瘤大小与深部穿支血管的关系可预测围手术期缺血性损伤,这是长期和永久性术后并发症最相关的危险因素。