Sema4, Stamford, Connecticut, USA.
Illinois CancerCare, Peoria, Illinois, USA.
Oncologist. 2021 Jul;26(7):e1226-e1239. doi: 10.1002/onco.13780. Epub 2021 May 11.
Racial disparities among clinical trial participants present a challenge to assess whether trial results can be generalized into patients representing diverse races and ethnicities. The objective of this study was to evaluate the impact of race and ethnicity on treatment response in patients with advanced non-small cell lung cancer (aNSCLC) treated with programmed cell death-1 (PD-1) or programmed cell death-ligand 1 (PD-L1) inhibitors through analysis of real-world data (RWD).
A retrospective cohort study of 11,138 patients with lung cancer treated at hospitals within the Mount Sinai Health System was performed. Patients with confirmed aNSCLC who received anti-PD-1/PD-L1 treatment were analyzed for clinical outcomes. Our cohort included 249 patients with aNSCLC who began nivolumab, pembrolizumab, or atezolizumab treatment between November 2014 and December 2018. Time-to-treatment discontinuation (TTD) and overall survival (OS) were the analyzed clinical endpoints.
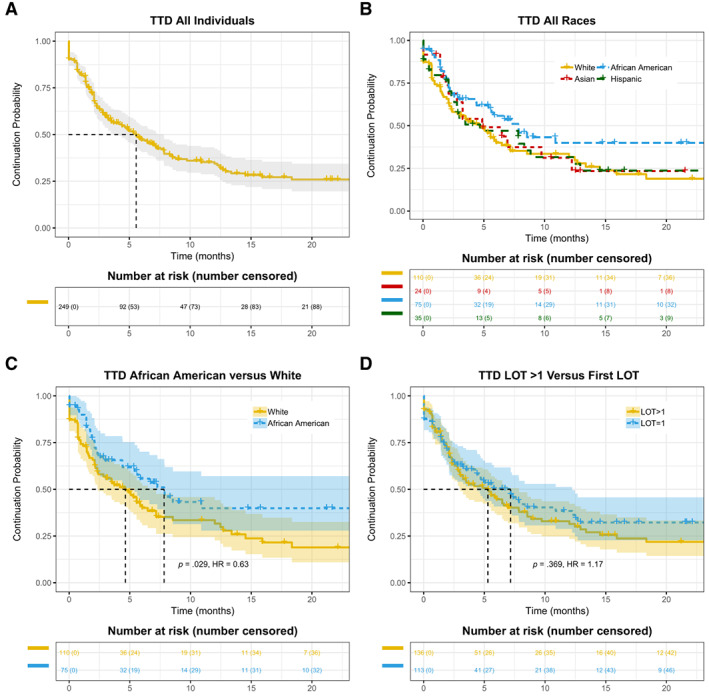
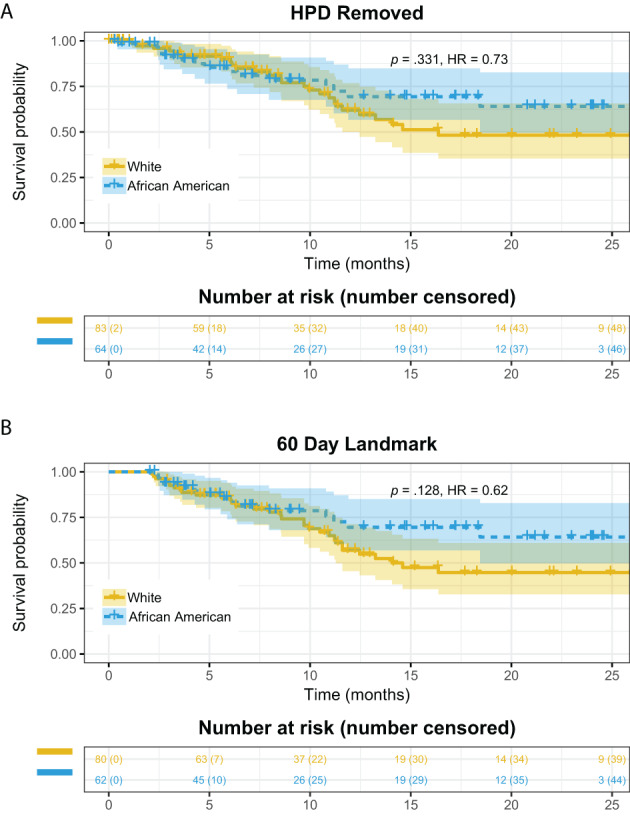
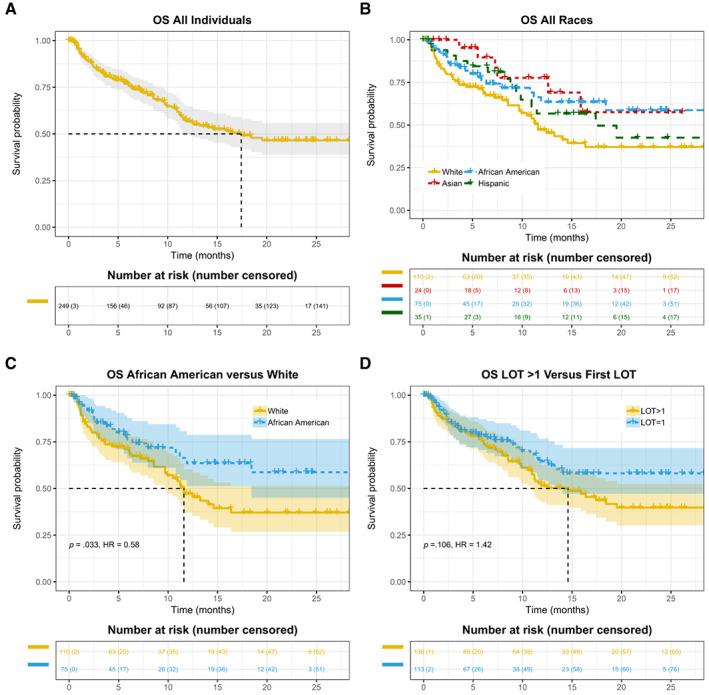
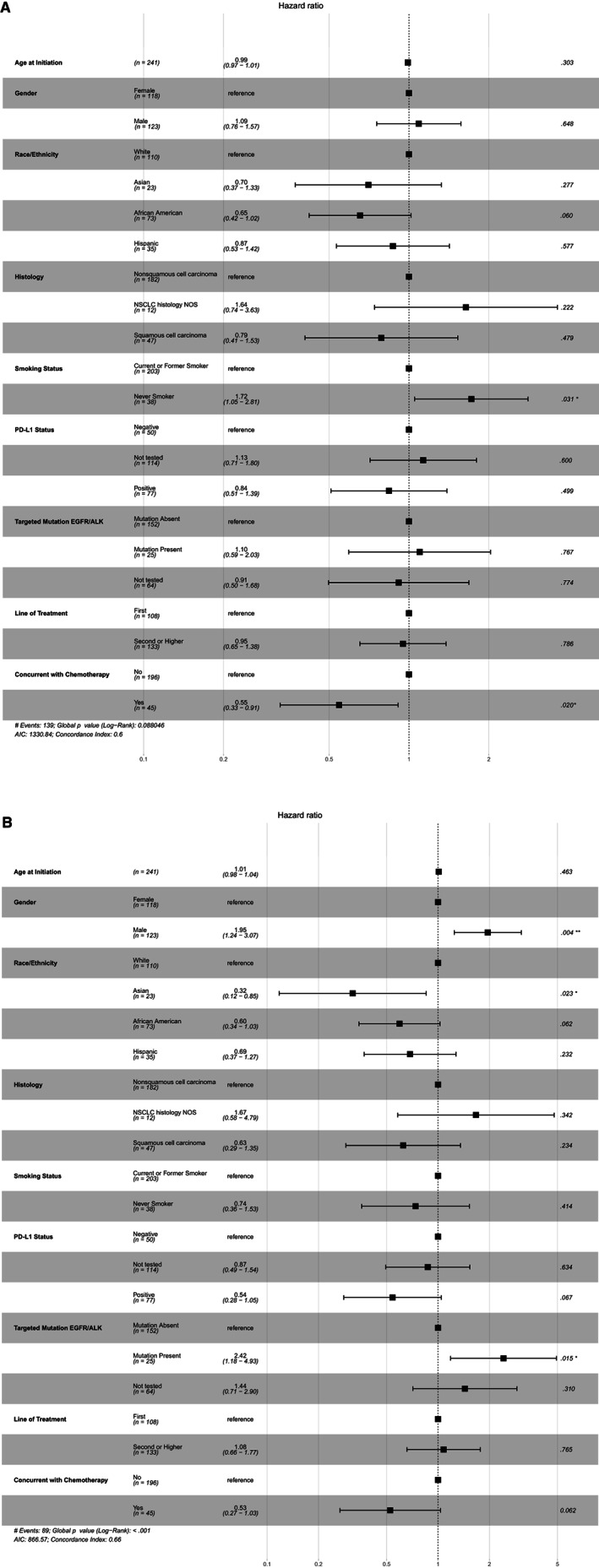
After a median follow-up of 14.8 months, median TTD was 7.8 months (95% confidence interval, 5.4-not estimable [NE]) in 75 African American patients versus 4.6 (2.4-7.2) in 110 White patients (hazard ratio [HR], 0.63). Median OS was not reached (18.4-NE) in African American patients versus 11.6 months (9.7-NE) in White patients (HR, 0.58). Multivariable Cox regression conducted with potential confounders confirmed longer TTD (adjusted HR, 0.65) and OS (adjusted HR, 0.60) in African American versus White patients. Similar real-world response rate (42.6% vs. 43.5%) and disease control rate (59.6% vs. 56.5%) were observed in the African American and White patient populations. Further investigation revealed the African American patient group had lower incidence (14.7%) of putative hyperprogressive diseases (HPD) upon anti-PD-1/PD-L1 treatment than the White patient group (24.5%).
Analysis of RWD showed longer TTD and OS in African American patients with aNSCLC treated with anti-PD-1/PD-L1 inhibitors. Lower incidence of putative HPD is a possible reason for the favorable outcomes in this patient population.
There is a significant underrepresentation of minority patients in randomized clinical trials, and this study demonstrates that real-world data can be used to investigate the impact of race and ethnicity on treatment response. In retrospective analysis of patients with advanced non-small cell lung cancer treated with programmed cell death-1 or programmed cell death-ligand 1 inhibitors, African American patients had significantly longer time-to-treatment discontinuation and longer overall survival. Analysis of real-world data can yield clinical insights and establish a more complete picture of medical interventions in routine clinical practice.
临床试验参与者中的种族差异对评估试验结果是否可推广至代表不同种族和族裔的患者构成了挑战。本研究的目的是通过对真实世界数据(RWD)的分析,评估种族和民族对接受程序性死亡受体-1(PD-1)或程序性死亡配体 1(PD-L1)抑制剂治疗的晚期非小细胞肺癌(aNSCLC)患者治疗反应的影响。
对在西奈山卫生系统医院就诊的 11138 例肺癌患者进行了一项回顾性队列研究。对接受抗 PD-1/PD-L1 治疗的确诊为 aNSCLC 患者的临床结局进行了分析。我们的队列包括 249 例于 2014 年 11 月至 2018 年 12 月期间开始接受纳武利尤单抗、帕博利珠单抗或阿特珠单抗治疗的 aNSCLC 患者。治疗中断时间(TTD)和总生存期(OS)是分析的临床终点。
中位随访 14.8 个月后,75 例非裔美国患者的中位 TTD 为 7.8 个月(95%置信区间,5.4-无法估计[NE]),110 例白人患者的中位 TTD 为 4.6(2.4-7.2)(风险比[HR],0.63)。非裔美国患者的中位 OS 未达到(18.4-NE),而白人患者的中位 OS 为 11.6 个月(9.7-NE)(HR,0.58)。对可能存在的混杂因素进行多变量 Cox 回归分析后,确认非裔美国患者的 TTD(调整 HR,0.65)和 OS(调整 HR,0.60)均长于白人患者。在非裔美国和白人患者人群中观察到相似的真实世界缓解率(42.6% vs. 43.5%)和疾病控制率(59.6% vs. 56.5%)。进一步的调查显示,接受抗 PD-1/PD-L1 治疗的非裔美国患者组中潜在 Hyperprogressive Disease(HPD)的发生率(14.7%)低于白人患者组(24.5%)。
对真实世界数据的分析表明,接受抗 PD-1/PD-L1 抑制剂治疗的非裔美国晚期 NSCLC 患者的 TTD 和 OS 更长。非裔美国患者组潜在 HPD 的发生率较低,这可能是该患者人群获得良好结局的原因。
在随机临床试验中,少数族裔患者的代表性严重不足,本研究表明,真实世界数据可用于研究种族和民族对治疗反应的影响。在接受程序性死亡受体 1 或程序性死亡配体 1 抑制剂治疗的晚期非小细胞肺癌患者的回顾性分析中,非裔美国患者的治疗中断时间和总生存期明显更长。对真实世界数据的分析可以产生临床见解,并更全面地了解常规临床实践中的医疗干预措施。