Department of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia.
Faculty of Medicine and Health Sciences, Universiti Sains Islam Malaysia, Nilai, Negeri Sembilan, Malaysia.
PLoS One. 2021 Apr 8;16(4):e0249592. doi: 10.1371/journal.pone.0249592. eCollection 2021.
IgA nephropathy (IgAN) has a heterogeneous presentation and the progression to end stage renal disease (ESRD) is often influenced by demographics, ethnicity, as well as choice of treatment regimen. In this study, we investigated the long term survival of IgAN patients in our center and the factors affecting it.
This study included all biopsy-proven IgAN patients with ≥ 1year follow-up. Patients with diabetes mellitus at diagnosis and secondary IgAN were excluded. Medical records were reviewed for demographics, clinical presentation, blood pressure, 24-hour urine protein, serum creatinine, renal biopsy and treatment received. The primary outcome was defined as combined event of 50% estimated glomerular filtration rate (eGFR) reduction or ESRD.
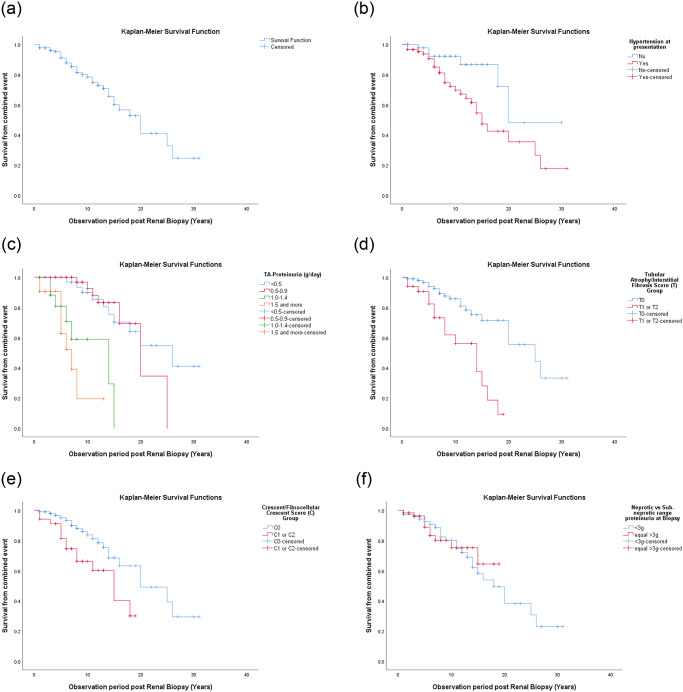
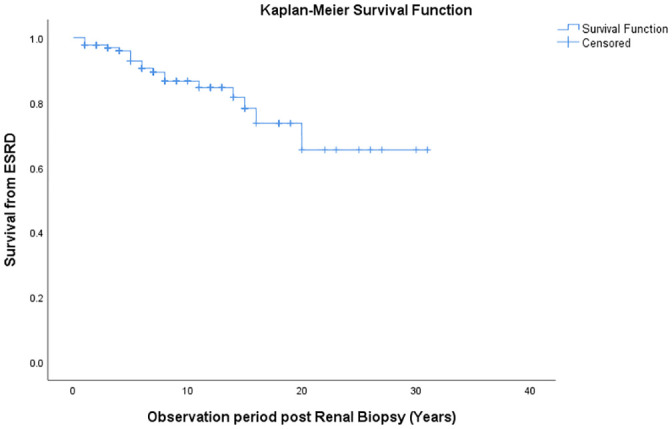
We included 130 (74 females; 56 males) patients of mean age 38.0 ± 14.0 years and median eGFR of 75.2 (interquartile range (IQR) 49.3-101.4) ml/min/1.73m2. Eighty-four (64.6%) were hypertensive at presentation, 35 (26.9%) had nephrotic syndrome and 57 (43.8%) had nephrotic range proteinuria (NRP). Median follow-up duration was 7.5 (IQR 4.0-13.0) years. It was noted that 18 (13.8%) developed ESRD and 34 (26.2%) reached the primary outcome. Annual eGFR decline was -2.1 (IQR -5.3 to -0.1) ml/min/1.73m2/year, with median survival of 20 years. Survival rates from the combined event (50% decrease in eGFR or ESRD) at 10, 20 and 30 years were 80%, 53% and 25%, while survival from ESRD were 87%, 73% and 65%, respectively. In the univariate analysis, time-average proteinuria (hazard ratio (HR) = 2.41, 95% CI 1.77-3.30), eGFR <45ml/min/1.73m2 at biopsy (HR = 2.35, 95% CI 1.03-5.32), hypertension (HR = 2.81, 95% CI 1.16-6.80), mean arterial pressure (HR = 1.02, 95% CI 1.01-1.04), tubular atrophy/interstitial fibrosis score (HR = 3.77, 95% CI 1.84-7.73), and cellular/fibrocellular crescent score (HR = 2.44, 95% CI 1.19-5.00) were found to be significant. Whereas only time-average proteinuria (TA-proteinuria) remained as a significant predictor in the multivariate analysis (HR = 2.23, 95% CI 1.57-3.16).
In our cohort, TA-proteinuria was the most important predictor in the progression of IgAN, irrespective of degree of proteinuria at presentation.
IgA 肾病 (IgAN) 表现具有异质性,向终末期肾病 (ESRD) 的进展通常受到人口统计学、种族以及治疗方案选择的影响。在本研究中,我们调查了我们中心 IgAN 患者的长期生存情况及其影响因素。
本研究纳入了所有随访时间≥1 年且经活检证实为 IgAN 的患者。排除了诊断时患有糖尿病和继发性 IgAN 的患者。回顾了患者的人口统计学、临床特征、血压、24 小时尿蛋白、血清肌酐、肾活检和接受的治疗等病历资料。主要结局定义为 eGFR 下降 50%或 ESRD 的复合事件。
我们纳入了 130 名(74 名女性;56 名男性)平均年龄为 38.0±14.0 岁、中位 eGFR 为 75.2(四分位距 (IQR) 49.3-101.4)ml/min/1.73m2 的患者。84 名(64.6%)患者在就诊时为高血压,35 名(26.9%)为肾病综合征,57 名(43.8%)为大量蛋白尿(NRP)。中位随访时间为 7.5(IQR 4.0-13.0)年。我们注意到,18 名(13.8%)患者发展为 ESRD,34 名(26.2%)患者达到了主要结局。每年 eGFR 下降速度为-2.1(IQR -5.3 至 -0.1)ml/min/1.73m2/年,中位生存时间为 20 年。10、20 和 30 年时联合事件(eGFR 下降 50%或 ESRD)的生存率分别为 80%、53%和 25%,而 ESRD 的生存率分别为 87%、73%和 65%。在单变量分析中,时间平均蛋白尿(危险比 (HR) = 2.41,95%置信区间 (CI) 1.77-3.30),活检时 eGFR <45ml/min/1.73m2(HR = 2.35,95% CI 1.03-5.32),高血压(HR = 2.81,95% CI 1.16-6.80),平均动脉压(HR = 1.02,95% CI 1.01-1.04),肾小管萎缩/间质纤维化评分(HR = 3.77,95% CI 1.84-7.73),细胞/纤维细胞新月体评分(HR = 2.44,95% CI 1.19-5.00)被发现是显著的。而只有时间平均蛋白尿(TA-蛋白尿)在多变量分析中仍然是一个重要的预测因素(HR = 2.23,95% CI 1.57-3.16)。
在我们的队列中,TA-蛋白尿是 IgAN 进展的最重要预测因素,而与就诊时蛋白尿的程度无关。