University of Virginia School of Medicine, Charlottesville, VA, United States of America.
Division of Cardiovascular Medicine, Department of Medicine, The Cardiovascular Imaging Center, University of Virginia Health System, Charlottesville, VA, United States of America.
PLoS One. 2021 Apr 8;16(4):e0249779. doi: 10.1371/journal.pone.0249779. eCollection 2021.
Exercise stress electrocardiography (ExECG) is recommended as a first-line tool to assess ischemia, but standard ST-analysis has limited diagnostic accuracy. ST elevation in lead aVR has been associated with left main and LAD disease in the population undergoing coronary angiography but has not been studied in the general population undergoing stress testing for the initial evaluation of CAD without coronary angiography. We sought to determine the predictive value of lead aVR elevation for ischemia, early revascularization, and subsequent cardiac events in consecutive patients undergoing ExECG.
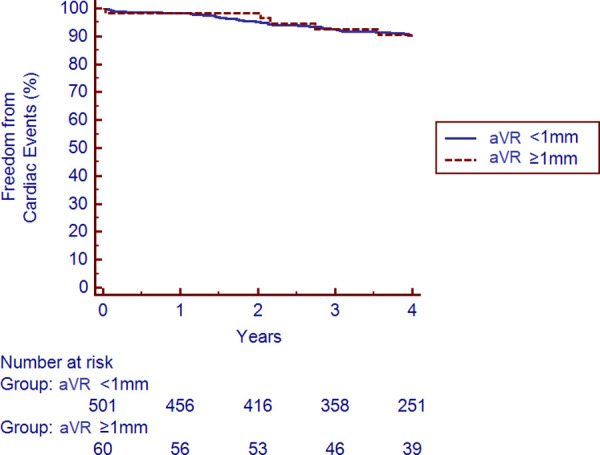
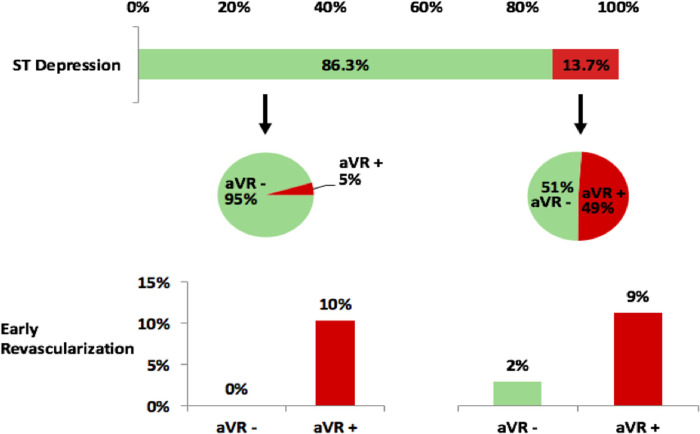
The study cohort included 641 subjects referred for ExECG who were dichotomized by presence or absence of aVR elevation ≥1mm and compared for prevalence and predictors of ischemia and a composite of cardiac death, nonfatal myocardial infarction, and late revascularization. The cohort had a median age of 57 and 57% were male. The prevalence of aVR elevation was 11.5%. The prevalence of significant ischemia on patients who received imaging was significantly higher with aVR elevation (14.3% vs 2.3%, p<0.001). Early revascularization occurred in 10.9% with vs 0.2% without aVR elevation, p<0.001. No subjects without aVR elevation or ST-depression underwent early revascularization. However, cardiac event rates were similar over a median 4.0 years of follow-up with and without aVR elevation (2.8% vs. 2.6%, p = 0.80). aVR elevation did not predict long-term cardiac events by Kaplan-Meier survival analysis (p = 0.94) or Cox proportional hazards modeling (p = 0.35).
aVR elevation during ExECG predicts ischemia on imaging and early revascularization but not long-term outcomes and could serve as a useful adjunct to standard ST-analysis and potentially reduce the need for concurrent imaging.
运动压力心电图(ExECG)被推荐作为评估缺血的一线工具,但标准 ST 分析的诊断准确性有限。在接受冠状动脉造影的人群中,aVR 导联的 ST 抬高与左主干和左前降支疾病相关,但在未接受冠状动脉造影的 CAD 初始评估中接受压力测试的一般人群中尚未进行研究。我们旨在确定 aVR 导联抬高对缺血、早期血运重建和随后的心脏事件的预测价值,在连续接受 ExECG 的患者中进行研究。
研究队列包括 641 例接受 ExECG 的患者,根据 aVR 抬高≥1mm 的存在与否分为两组,并比较两组缺血和心脏死亡、非致死性心肌梗死和晚期血运重建的复合终点的发生率和预测因素。该队列的中位年龄为 57 岁,57%为男性。aVR 抬高的患病率为 11.5%。接受影像学检查的患者中,aVR 抬高患者的显著缺血患病率明显较高(14.3% vs 2.3%,p<0.001)。早期血运重建分别在 10.9%和 0.2%的患者中发生,aVR 抬高组明显高于无 aVR 抬高组(p<0.001)。无 aVR 抬高或 ST 压低的患者均未进行早期血运重建。然而,中位随访 4.0 年期间,aVR 抬高组和无 aVR 抬高组的心脏事件发生率相似(2.8% vs. 2.6%,p=0.80)。Kaplan-Meier 生存分析(p=0.94)和 Cox 比例风险模型(p=0.35)均未显示 aVR 抬高预测长期心脏事件。
ExECG 期间的 aVR 抬高可预测影像学检查中的缺血和早期血运重建,但不能预测长期结局,可作为标准 ST 分析的有用辅助手段,并可能减少同时进行影像学检查的需求。