Ladapo Joseph A, Blecker Saul, Douglas Pamela S
Ann Intern Med. 2014 Oct 7;161(7):482-90. doi: 10.7326/M14-0296.
Cardiac stress testing, particularly with imaging, has been the focus of debates about rising health care costs, inappropriate use, and patient safety in the context of radiation exposure.
To determine whether U.S. trends in cardiac stress test use may be attributable to population shifts in demographics, risk factors, and provider characteristics and evaluate whether racial/ethnic disparities exist in physician decision making.
Analyses of repeated cross-sectional data.
National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey (1993 to 2010).
Adults without coronary heart disease.
Cardiac stress test referrals and inappropriate use.
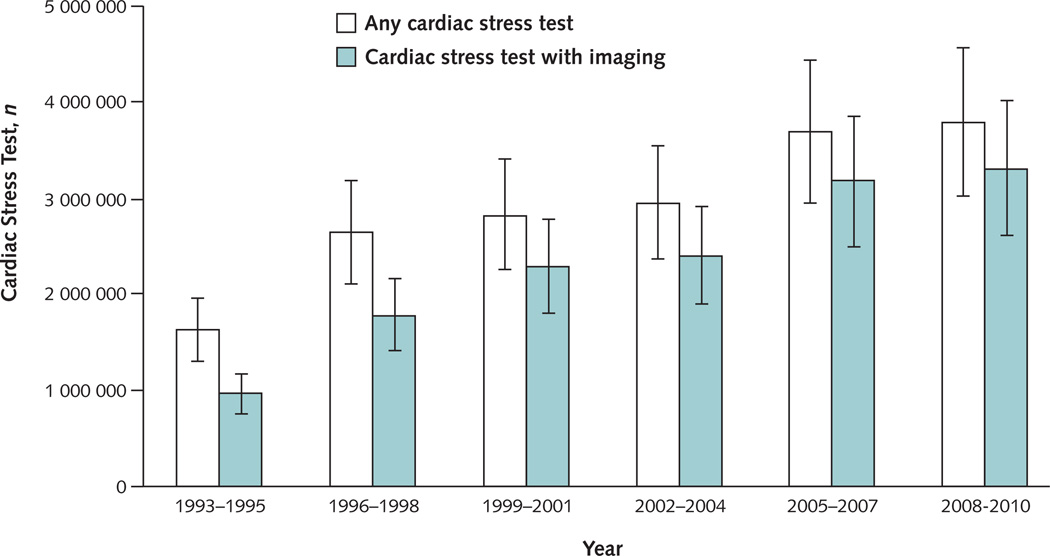
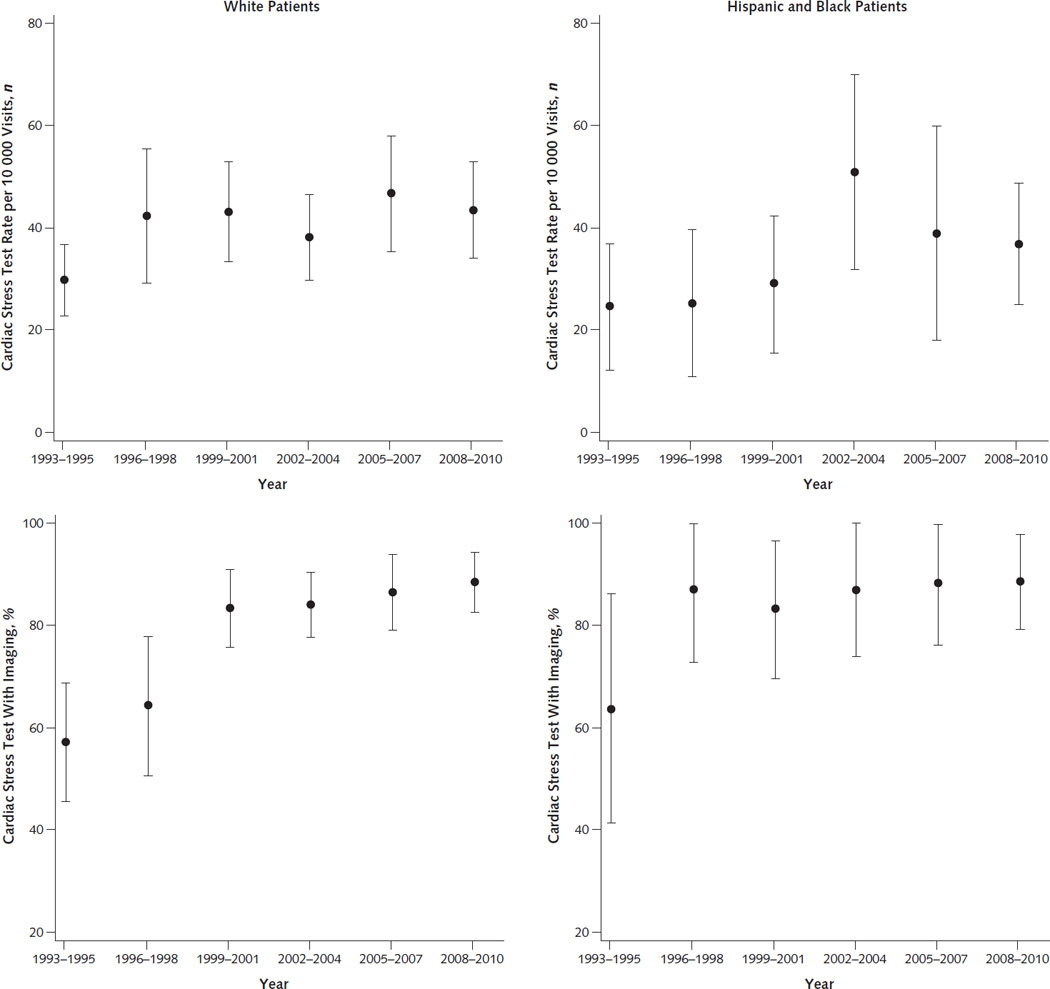
Between 1993 to 1995 and 2008 to 2010, the annual number of U.S. ambulatory visits in which a cardiac stress test was ordered or performed increased from 28 per 10,000 visits to 45 per 10,000 visits. No trend was found toward more frequent testing after adjustment for patient characteristics, risk factors, and provider characteristics (P = 0.134). Cardiac stress tests with imaging comprised a growing portion of all tests, increasing from 59% in 1993 to 1995 to 87% in 2008 to 2010. At least 34.6% were probably inappropriate, with associated annual costs and harms of $501 million and 491 future cases of cancer. Authors found no evidence of a lower likelihood of black patients receiving a cardiac stress test (odds ratio, 0.91 [95% CI, 0.69 to 1.21]) than white patients, although some evidence of disparity in Hispanic patients was found (odds ratio, 0.75 [CI, 0.55 to 1.02]).
Cross-sectional design with limited clinical data.
National growth in cardiac stress test use can largely be explained by population and provider characteristics, but use of imaging cannot. Physician decision making about cardiac stress test use does not seem to contribute to racial/ethnic disparities in cardiovascular disease.
National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences.
心脏应激试验,尤其是结合成像技术的试验,一直是关于医疗保健成本上升、使用不当以及辐射暴露情况下患者安全等问题争论的焦点。
确定美国心脏应激试验使用趋势是否可归因于人口统计学、风险因素和医疗服务提供者特征的变化,并评估医生决策中是否存在种族/民族差异。
对重复横断面数据进行分析。
国家门诊医疗调查和国家医院门诊医疗调查(1993年至2010年)。
无冠心病的成年人。
心脏应激试验转诊情况及使用不当情况。
在1993年至1995年与2008年至2010年期间,美国门诊中开具或进行心脏应激试验的年度就诊次数从每10000次就诊28次增加到每10000次就诊45次。在对患者特征、风险因素和医疗服务提供者特征进行调整后,未发现更频繁进行试验的趋势(P = 0.134)。结合成像技术的心脏应激试验在所有试验中所占比例不断增加,从1993年至1995年的59%增至2008年至2010年的87%。至少34.6%的试验可能是不恰当的,相关年度成本和危害分别为5.01亿美元和未来491例癌症病例。作者未发现黑人患者接受心脏应激试验的可能性低于白人患者的证据(优势比,0.91 [95%可信区间,0.69至1.21]),不过发现西班牙裔患者存在一些差异的证据(优势比,0.75 [可信区间,0.55至1.02])。
横断面设计且临床数据有限。
美国心脏应激试验使用的全国性增长在很大程度上可由人口和医疗服务提供者特征来解释,但成像技术的使用并非如此。医生在心脏应激试验使用方面的决策似乎并未导致心血管疾病中的种族/民族差异。
国家心肺血液研究所和国家推进转化科学中心。