Department of General, Visceral, Vascular, and Transplant Surgery, University Hospital Magdeburg, Leipziger Strasse 44, 39120, Magdeburg, Germany.
Centre Hospitalier Intercommunal de Poissy/Saint-Germain-En-Laye, 10 Rue du Champ Gaillard, 78300, Poissy, France.
Langenbecks Arch Surg. 2021 May;406(3):753-761. doi: 10.1007/s00423-021-02152-6. Epub 2021 Apr 8.
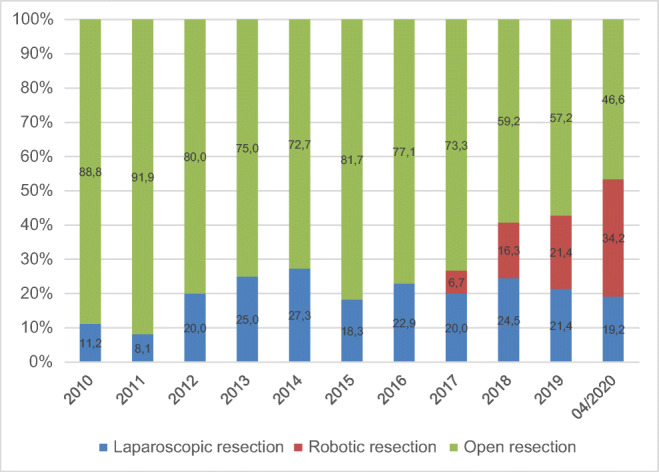
Minimally invasive liver surgery (MILS) is a feasible and safe procedure for benign and malignant tumors. There has been an ongoing debate on whether conventional laparoscopic liver resection (LLR) or robotic liver resection (RLR) is superior and if one approach should be favored over the other. We started using LLR in 2010, and introduced RLR in 2013. In the present paper, we report on our experiences with these two techniques as early adopters in Germany.
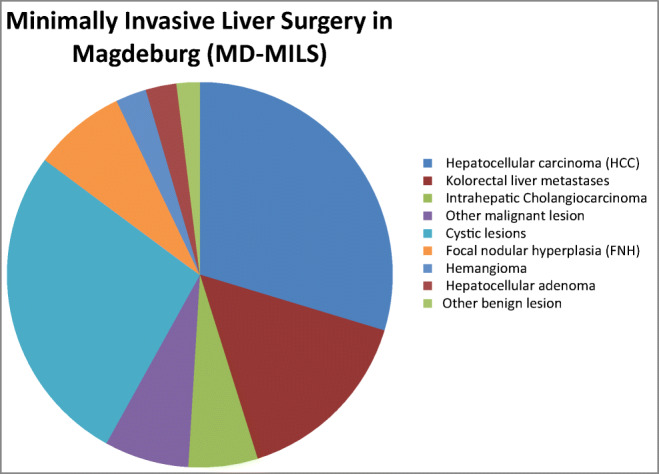
The data of patients who underwent MILS between 2010 and 2020 were collected prospectively in the Magdeburg Registry for Minimally Invasive Liver Surgery (MD-MILS). A retrospective analysis was performed regarding patient demographics, tumor characteristics, and perioperative parameters.
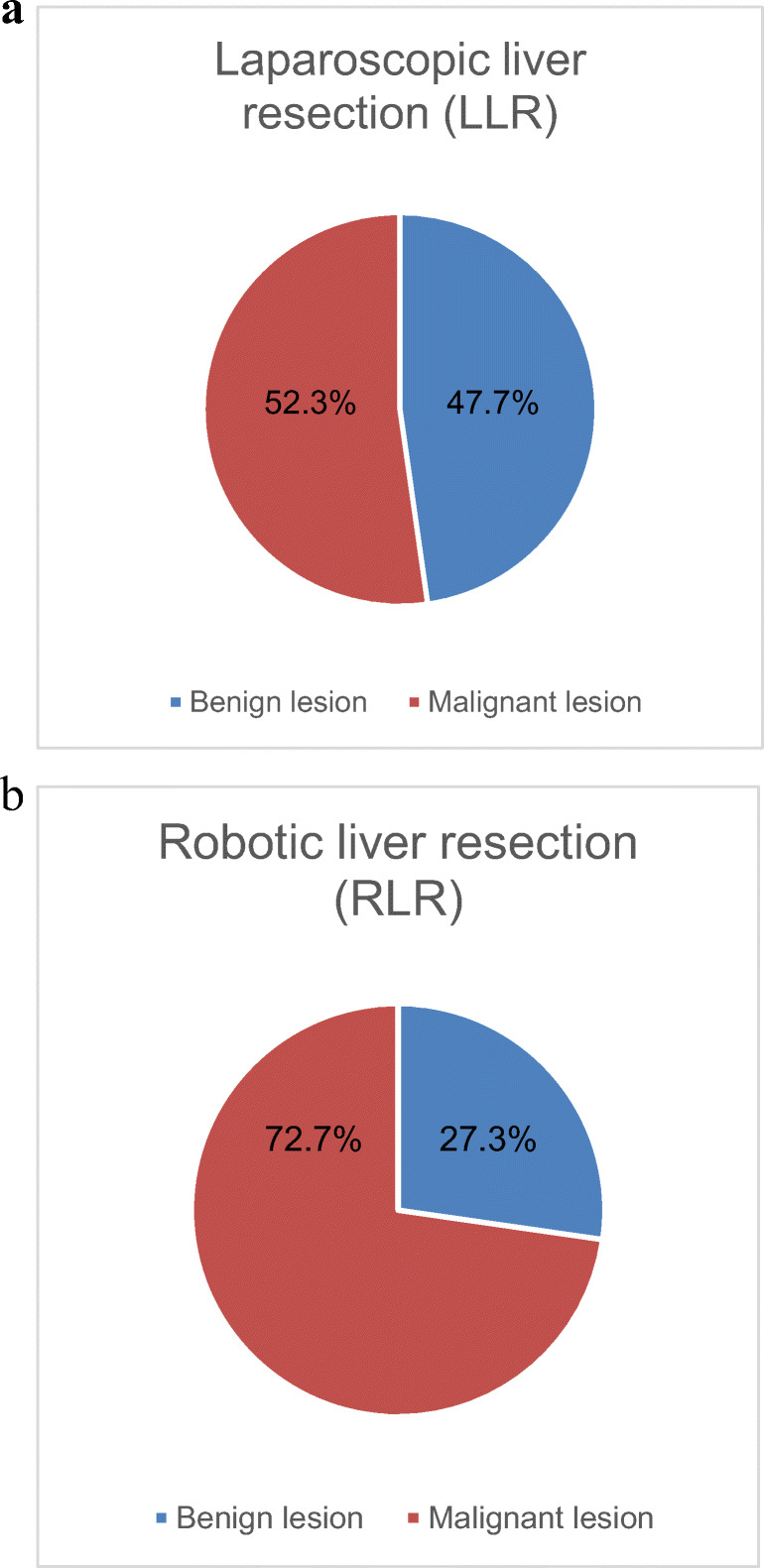
We identified 155 patients fulfilling the inclusion criteria. Of these, 111 (71.6%) underwent LLR and 44 (29.4%) received RLR. After excluding cystic lesions, 113 cases were used for the analysis of perioperative parameters. Resected specimens were significantly bigger in the RLR vs. the LLR group (405 g vs. 169 g, p = 0.002); in addition, the tumor diameter was significantly larger in the RLR vs. the LLR group (5.6 cm vs. 3.7 cm, p = 0.001). Hence, the amount of major liver resections (three or more segments) was significantly higher in the RLR vs. the LLR group (39.0% vs. 16.7%, p = 0.005). The mean operative time was significantly longer in the RLR vs. the LLR group (331 min vs. 181 min, p = 0.0001). The postoperative hospital stay was significantly longer in the RLR vs. the LLR group (13.4 vs. LLR 8.7 days, p = 0.03). The R0 resection rate for solid tumors was higher in the RLR vs. the LLR group but without statistical significance (93.8% vs. 87.9%, p = 0.48). The postoperative morbidity ≥ Clavien-Dindo grade 3 was 5.6% in the LLR vs. 17.1% in the RLR group (p = 0.1). No patient died in the RLR but two patients (2.8%) died in the LLR group, 30 and 90 days after surgery (p = 0.53).
Minimally invasive liver surgery is safe and feasible. Robotic and laparoscopic liver surgery shows similar and adequate perioperative oncological results for selected patients. RLR might be advantageous for more advanced and technically challenging procedures.
微创肝切除术(MILS)是治疗良性和恶性肿瘤的一种可行且安全的方法。对于传统腹腔镜肝切除术(LLR)和机器人肝切除术(RLR)哪种更优越,以及是否应该优先选择其中一种方法,一直存在争议。我们于 2010 年开始使用 LLR,并于 2013 年引入 RLR。在本文中,我们作为德国的早期采用者,报告了这两种技术的经验。
前瞻性地收集了 2010 年至 2020 年间接受 MILS 的患者数据,并将其纳入 Magdeburg 微创肝外科登记处(MD-MILS)。回顾性分析了患者的人口统计学、肿瘤特征和围手术期参数。
我们确定了 155 名符合纳入标准的患者。其中,111 名(71.6%)接受了 LLR,44 名(29.4%)接受了 RLR。在排除囊性病变后,对 113 例患者的围手术期参数进行了分析。RLR 组的切除标本明显大于 LLR 组(405 克比 169 克,p = 0.002);此外,RLR 组的肿瘤直径明显大于 LLR 组(5.6 厘米比 3.7 厘米,p = 0.001)。因此,RLR 组的主要肝切除术(三个或更多节段)明显高于 LLR 组(39.0%比 16.7%,p = 0.005)。RLR 组的手术时间明显长于 LLR 组(331 分钟比 181 分钟,p = 0.0001)。RLR 组的术后住院时间明显长于 LLR 组(13.4 天比 LLR 组的 8.7 天,p = 0.03)。RLR 组的实体瘤 R0 切除率高于 LLR 组,但无统计学意义(93.8%比 87.9%,p = 0.48)。LR 组的术后发病率≥Clavien-Dindo 3 级为 5.6%,而 RLR 组为 17.1%(p = 0.1)。RLR 组无患者死亡,但 LLR 组有 2 例患者(2.8%)死亡,分别在术后 30 天和 90 天(p = 0.53)。
微创肝切除术是安全可行的。机器人和腹腔镜肝切除术对选定患者的围手术期肿瘤学结果相似且足够。RLR 可能对更先进和技术更具挑战性的手术有益。