Egoryan Goar, Murguia-Fuentes Ricardo, Agab Mohamed, Abou-Ghanem Nagwa, Yanez-Bello Maria Adriana, Pyakuryal Bimatshu, Trelles-Garcia Daniela Patricia, Ibrahim Rami, Filipiuk Dorota, Gidron Adi, Rodriguez-Nava Guillermo
Department of Internal Medicine, AMITA Health Saint Francis Hospital, 355 Ridge Ave, Evanston, IL, 60202, USA.
Department of Neurology, Louisiana State University Health Sciences Center, Shreveport, LA, USA.
J Med Case Rep. 2021 Apr 12;15(1):161. doi: 10.1186/s13256-021-02780-y.
Posterior reversible encephalopathy syndrome (PRES) is a clinical-radiologic entity characterized by headaches, altered mental status, seizures, visual loss, and a characteristic imaging pattern in brain magnetic resonance images. The exact etiology and pathogenesis of this condition are not yet fully elucidated.
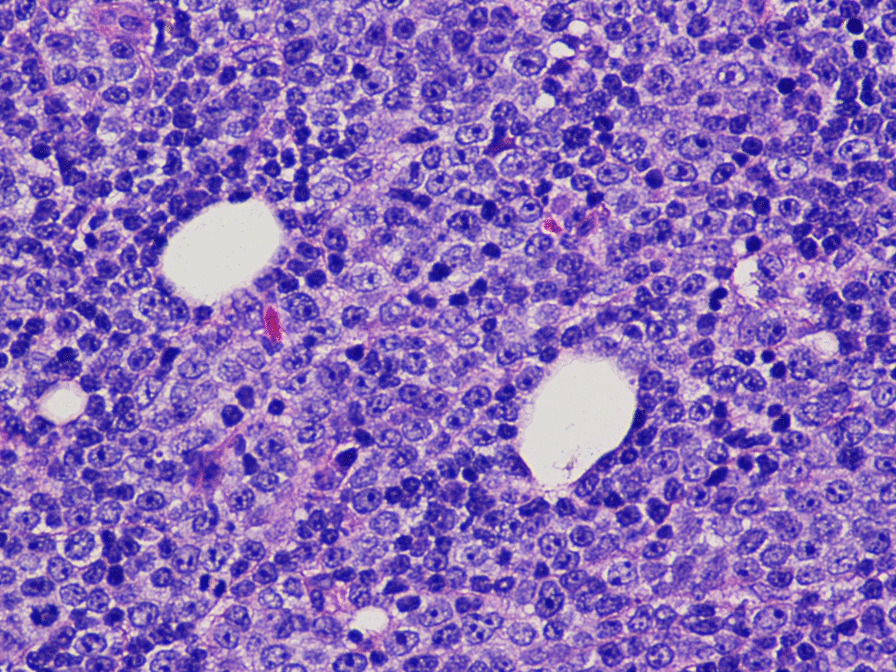
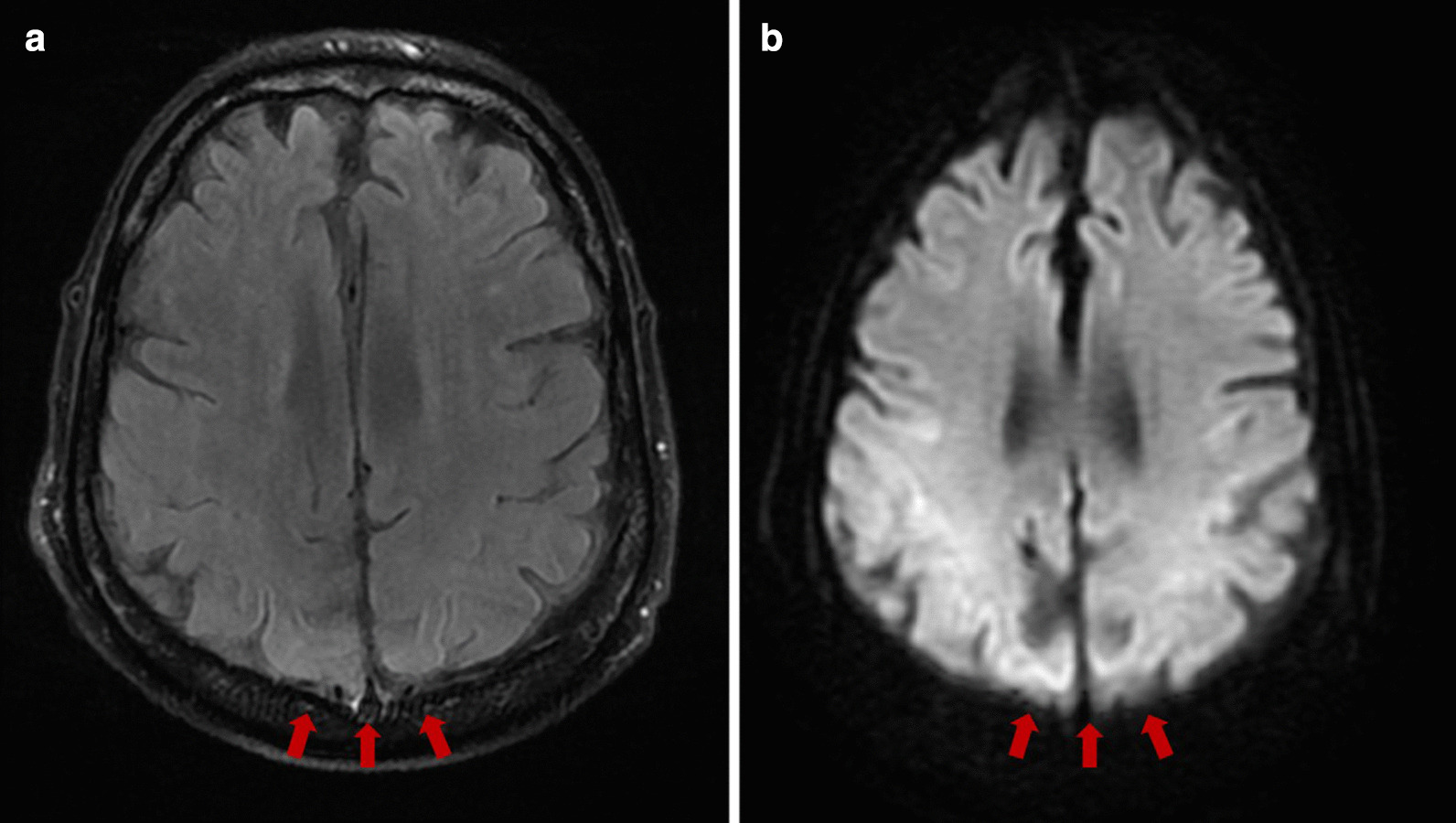
A 72-year-old White man presented with 2 weeks of low-grade fever and chills, night sweats, fatigue, dysphagia, and new-onset rapidly increasing cervical lymphadenopathy. He had a history of chronic lymphocytic leukemia with transformation to diffuse large B-cell lymphoma for which he was started on dose-adjusted rituximab, etoposide, prednisone vincristine, cyclophosphamide, and doxorubicin (DA-R-EPOCH). Shortly after treatment initiation, the patient developed severe airway obstruction due to cervical lymphadenopathy that required emergency intubation. A few days later, the cervical lymphadenopathy and the status of the airway improved, and sedation was consequently weaned off to plan for extubation. However, the patient did not recover consciousness and developed generalized refractory seizures. Brain magnetic resonance imaging revealed edema in the cortical gray and subcortical white matter of the bilateral occipital and inferior temporal lobes, consistent with PRES.
Posterior reversible encephalopathy syndrome refers to a neurological disorder and imaging entity characterized by subcortical vasogenic edema in patients who develop acute neurological signs and symptoms of a usually reversible nature in different settings, including chemotherapy. Despite its name, PRES is not always fully reversible, and permanent sequelae can persist in some patients. Clinicians should be aware of the possible association between chemotherapy and PRES to ensure early recognition and timely treatment.
后部可逆性脑病综合征(PRES)是一种临床-影像学实体,其特征为头痛、精神状态改变、癫痫发作、视力丧失以及脑磁共振成像中的特征性影像表现。这种疾病的确切病因和发病机制尚未完全阐明。
一名72岁白人男性,出现持续2周的低热、寒战、盗汗、疲劳、吞咽困难以及新发的迅速增大的颈部淋巴结病。他有慢性淋巴细胞白血病病史,已转化为弥漫性大B细胞淋巴瘤,为此他开始接受剂量调整的利妥昔单抗、依托泊苷、泼尼松、长春新碱、环磷酰胺和阿霉素(DA-R-EPOCH)治疗。治疗开始后不久,患者因颈部淋巴结病出现严重气道阻塞,需要紧急插管。几天后,颈部淋巴结病和气道状况改善,随后停用镇静剂以计划拔管。然而,患者未恢复意识并出现全身性难治性癫痫发作。脑磁共振成像显示双侧枕叶和颞下叶皮质灰质和皮质下白质水肿,符合PRES表现。
后部可逆性脑病综合征是指一种神经疾病和影像学实体,其特征为在不同情况下(包括化疗)出现急性神经体征和症状(通常具有可逆性)的患者发生皮质下血管源性水肿。尽管其名称如此,但PRES并非总是完全可逆,一些患者可能会遗留永久性后遗症。临床医生应意识到化疗与PRES之间可能存在的关联,以确保早期识别和及时治疗。