Song Andrew J, Evans Nathaniel, Cowan Scott, Guo Jenny, Zhan Tingting, Lu Bo, Werner-Wasik Maria
Department of Radiation Oncology, Sidney Kimmel Cancer Center, Thomas Jefferson University, Philadelphia, PA, USA.
Department of Surgery, Division of Thoracic Surgery, Thomas Jefferson University, Philadelphia, PA, USA.
J Thorac Dis. 2021 Mar;13(3):1576-1583. doi: 10.21037/jtd-20-2001.
Virtually all patients with medically inoperable stage I non-small cell lung cancer (NSCLC) can receive stereotactic body radiation therapy. However, the percentage of such patients in whom sublobar resection is technically feasible is unknown. This discrepancy can confound clinical trial eligibility and designs comparing stereotactic body radiation therapy . sublobar resection.
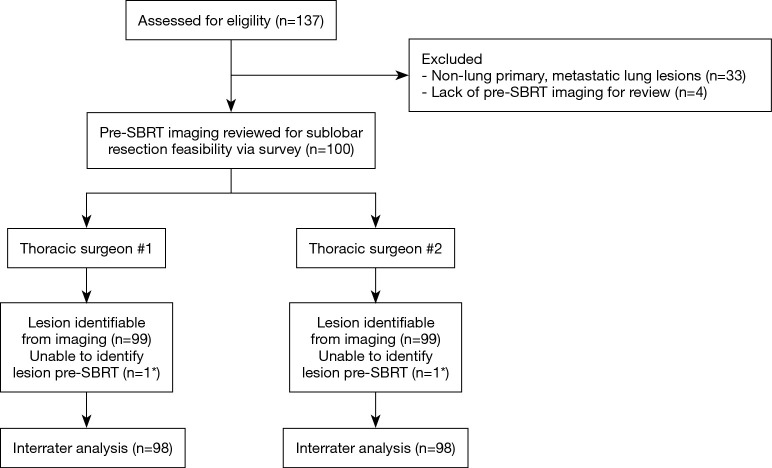
A total of 137 patients treated with stereotactic body radiation therapy for lung lesions (3/2013-11/2017) underwent retrospective review. Diagnostic CT chest and PET/CT images, stereotactic body radiation therapy dates, and demographic data were collected on 100 of 137 patients. Two experienced board-certified thoracic surgeons independently reviewed anonymized patients' pre-stereotactic body radiation therapy diagnostic imaging and completed a custom survey about the technical feasibility of sublobar resection for each patient. Interrater agreement was measured using Cohen's kappa coefficient by bootstrap methodology. Summary statistics were performed for baseline demographics and tumor characteristics.
Of the 100 patients, 57% were female, with median age of 75 years (range, 52-95 years) and Karnofsky Performance Status of 80 (range, 40-100). Most patients (61%) had Stage IA1, T1a tumors. For interrater agreement analysis, one patient was removed from each cohort due to inability to locate tumor on images, leaving 98 patients analyzed. Comparing Surgeon #1 . Surgeon #2, 64 (65.3%) . 69 (70.3%) of tumors were thought eligible for sublobar resection, respectively (κ=0.414).
Stereotactic body radiation therapy for stage I NSCLC is applicable to more tumors than sublobar resection, with ~30-35% of stereotactic body radiation therapy patients unable to undergo sublobar resection assessed by pretreatment diagnostic imaging based on technical grounds. This study illustrates that clinical trials comparing stereotactic body radiation therapy . sublobar resection are limited to only a subpopulation of patients with stage I NSCLC.
几乎所有医学上无法手术的I期非小细胞肺癌(NSCLC)患者都可接受立体定向体部放疗。然而,技术上可行肺叶下切除的此类患者的比例尚不清楚。这种差异可能会混淆临床试验的入选标准以及比较立体定向体部放疗与肺叶下切除的试验设计。
对2013年3月至2017年11月期间接受立体定向体部放疗治疗肺部病变的137例患者进行回顾性分析。收集了137例患者中100例的胸部诊断CT和PET/CT图像、立体定向体部放疗日期及人口统计学数据。两名经验丰富的经委员会认证的胸外科医生独立回顾了患者立体定向体部放疗前的匿名诊断影像,并完成了一项关于每位患者肺叶下切除技术可行性的定制调查。采用自抽样法通过Cohen卡方系数测量评分者间的一致性。对基线人口统计学和肿瘤特征进行了汇总统计。
100例患者中,57%为女性,中位年龄75岁(范围52 - 95岁),卡氏功能状态评分80(范围40 - 100)。大多数患者(61%)为IA1期、T1a肿瘤。在评分者间一致性分析中,由于在影像上无法定位肿瘤,每个队列各剔除1例患者,最终分析98例患者。比较外科医生1和外科医生2的评估结果,分别有64例(65.3%)和69例(70.3%)肿瘤被认为适合肺叶下切除(κ = 0.414)。
I期NSCLC的立体定向体部放疗适用于比肺叶下切除更多的肿瘤,约30% - 35%接受立体定向体部放疗的患者基于技术原因经预处理诊断影像评估无法进行肺叶下切除。本研究表明,比较立体定向体部放疗与肺叶下切除的临床试验仅局限于I期NSCLC患者的一个亚组。