Sandhu Avnish, Korzeniewski Steven J, Polistico Jordan, Pinnamaneni Harshita, Reddy Sushmitha Nanja, Oudeif Ahmed, Meyers Jessica, Sidhu Nikki, Levy Phillip, Samavati Lobelia, Badr M Safwan, Sobel Jack D, Sherwin Robert, Chopra Teena
Department of Internal Medicine, Division of Infectious Diseases, Detroit Medical Center, Wayne State University School of Medicine, Detroit, MI, United States.
Department of Family Medicine and Public Health Sciences, Wayne State University School of Medicine, Detroit, MI, United States.
EClinicalMedicine. 2021 Apr;34:100814. doi: 10.1016/j.eclinm.2021.100814. Epub 2021 Apr 6.
the incidence of novel coronavirus disease (COVID19) is elevated in areas with heightened socioeconomic vulnerability. Early reports from US hospitals also implicated social disadvantage and chronic disease history as COVID19 mortality risk factors. However, the relationship between race and COVID19 mortality remains unclear.
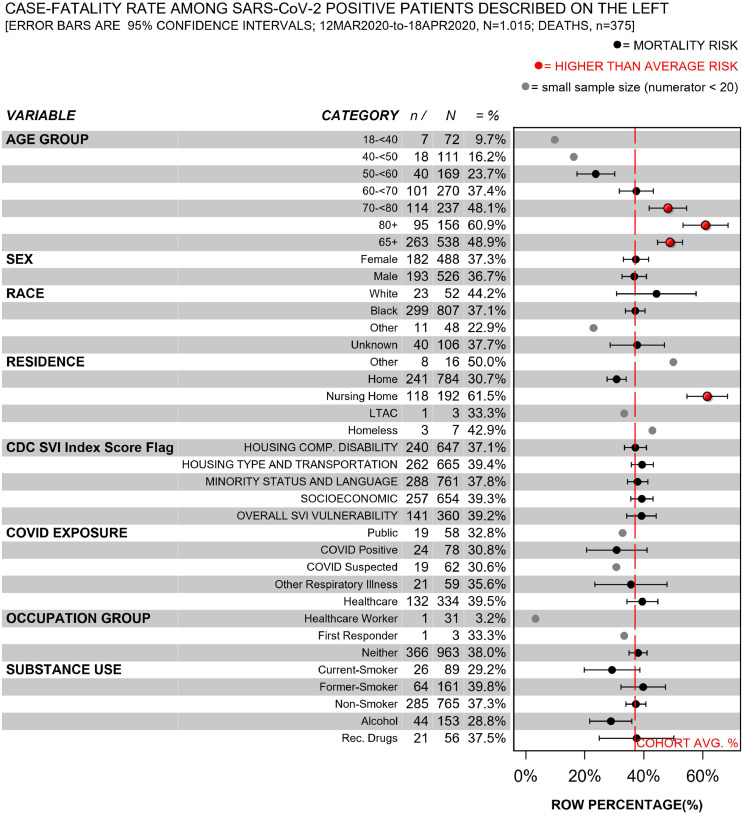
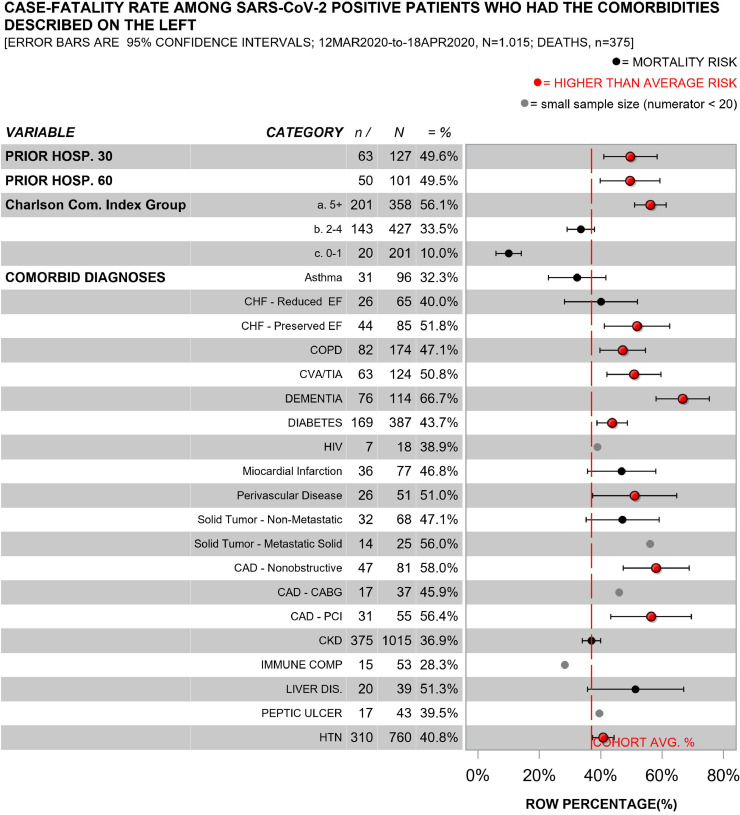
we examined in-hospital COVID19 mortality risk factors in a multi-hospital tertiary health care system that serves greater Detroit, Michigan, a predominantly African American city with high rates of poverty and chronic disease. Consecutive adult patients who presented to emergency departments and tested positive for COVID19 from 3/11/2020 through 4/18/2020 were included. Using log-binomial regression, we assessed the relationship between in-hospital mortality and residence in census tracts that were flagged for extreme socioeconomic vulnerability, patient-level demographics, and clinical comorbidities.
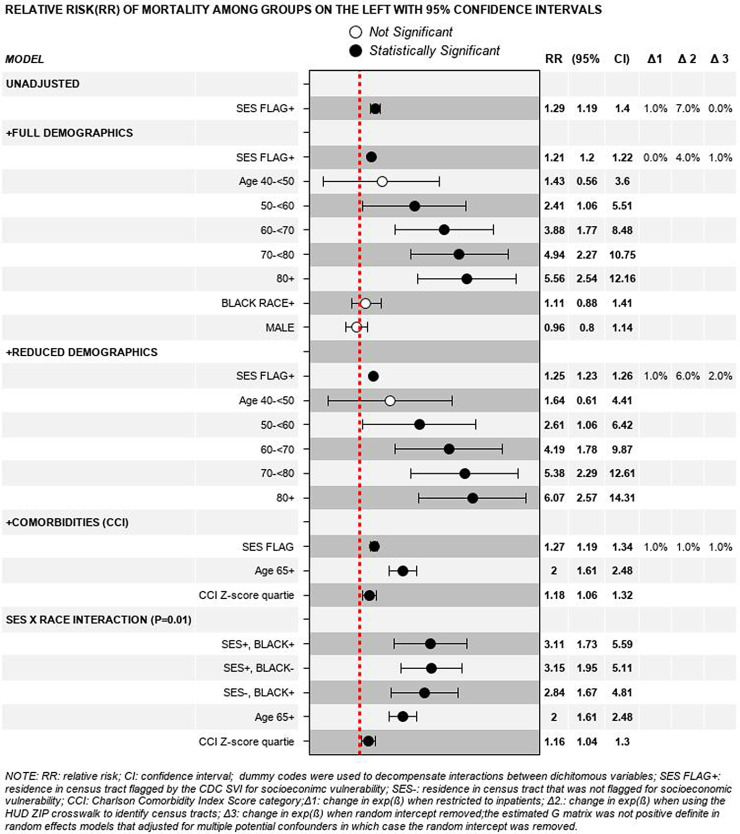
a total of 1,015 adults tested positive for COVID19 during the study period; 80% identified as Black people, 52% were male and 53% were ≥ 65 years of age. The median body mass index was 30•4 and the median Charlson Comorbidity Index score was 4. Patients from census tracts that were flagged for vulnerability related to socioeconomic status had a higher mortality rate than their peers who resided in less vulnerable census tracts (β 0.26, standard error (SE) 0.11, degrees of freedom (df) 378, -value () 2.27, exp(β) 1.29, -value 0.02). Adjustment for age category, Black race, sex and/or the Charlson Comorbidity Index score category reduced the magnitude of association by less than 10% [exp(β) 1.29 vs. 1.21]. Black race [ = 0.38] and sex [ = 0.62] were not associated with mortality in this sample.
people who lived in areas flagged for extreme socioeconomic vulnerability had elevated mortality risk in our predominantly African-American cohort of COVID19 patients who were able to seek hospital care during the so-called 'first wave' of the pandemic. By contrast, Black race was not associated with mortality in our sample.
在社会经济脆弱性较高的地区,新型冠状病毒病(COVID-19)的发病率有所上升。美国医院的早期报告也指出,社会劣势和慢性病病史是COVID-19的死亡风险因素。然而,种族与COVID-19死亡率之间的关系仍不明确。
我们在一个为密歇根州底特律市提供服务的多医院三级医疗保健系统中,研究了住院COVID-19患者的死亡风险因素。底特律是一个以非裔美国人为主的城市,贫困率和慢性病发病率都很高。纳入了2020年3月11日至2020年4月18日期间到急诊科就诊并COVID-19检测呈阳性的连续成年患者。我们使用对数二项回归,评估了住院死亡率与被标记为极端社会经济脆弱性的人口普查区居住情况、患者层面的人口统计学特征以及临床合并症之间的关系。
在研究期间,共有1015名成年人COVID-19检测呈阳性;80%为黑人,52%为男性,53%年龄≥65岁。体重指数中位数为30.4,查尔森合并症指数评分中位数为4。来自被标记为与社会经济地位相关的脆弱性人口普查区的患者,其死亡率高于居住在脆弱性较低的人口普查区的同龄人(β为0.26,标准误(SE)为0.11,自由度(df)为378,P值为2.27,exp(β)为1.29,P值为0.02)。对年龄类别、黑人种族、性别和/或查尔森合并症指数评分类别进行调整后,关联强度降低不到10%[exp(β)为1.29对1.21]。在该样本中,黑人种族(P = 0.38)和性别(P = 0.62)与死亡率无关。
在我们这个以非裔美国人为主的COVID-19患者队列中,即那些在疫情所谓的“第一波”期间能够寻求医院治疗的患者中,居住在被标记为极端社会经济脆弱性地区的人死亡风险升高。相比之下,在我们的样本中,黑人种族与死亡率无关。