Department of General - and Visceral Surgery, Medical Center-University of Freiburg, Hugstetterstrasse 55, 79106, Freiburg, Germany.
Department of Diagnostic and Interventional Radiology, Medical Center-University of Freiburg, Hugstetterstrasse 55, 79106, Freiburg, Germany.
World J Surg. 2021 Jul;45(7):2218-2226. doi: 10.1007/s00268-021-06073-9. Epub 2021 Apr 11.
The impact of body compositions on surgical results is controversially discussed. This study examined whether visceral obesity, sarcopenia or sarcopenic obesity influence the outcome after hepatic resections of synchronous colorectal liver metastases.
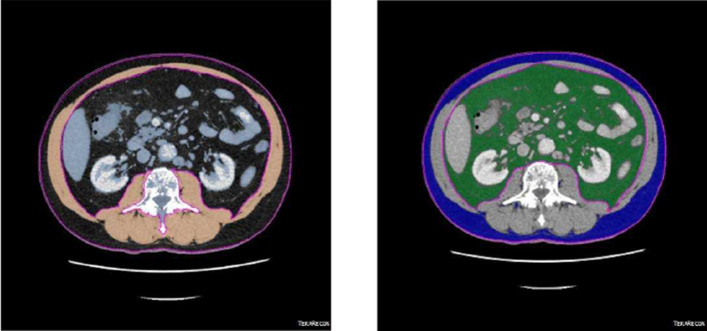
Ninety-four consecutive patients with primary hepatic resections of synchronous colorectal metastases were identified from a single center database between January 2013 and August 2018. Patient characteristics and 30-day morbidity were retrospectively analyzed. Body fat and skeletal muscle were calculated by planimetry from single-slice CT images at the level of L3.
Fifty-nine patients (62.8%) underwent minor hepatectomies, and 35 patients underwent major resections (37.2%). Postoperative complications occurred in 60 patients (62.8%) including 35 patients with major complications (Clavien-Dindo grade III-V). The mortality was nil at 30 days and 2.1% at 90 days. The body mass index showed no influence on postoperative outcomes (p = 1.0). Visceral obesity was found in 66 patients (70.2%) and was significantly associated with overall and major complication rates (p = .002, p = .012, respectively). Sarcopenia was observed in 34 patients (36.2%) without a significant impact on morbidity (p = .461), however, with longer hospital stay. Sarcopenic obesity was found in 18 patients (19.1%) and was significantly associated with postoperative complications (p = .014). Visceral obesity, sarcopenia and sarcopenic obesity were all identified as significant risk factors for overall postoperative complications.
Visceral obesity, sarcopenic obesity and sarcopenia are independent risk factors for overall complications after resections of CRLM. Early recognition of extremes in body compositions could prompt to perioperative interventions and thus improve postoperative outcomes.
身体成分对手术结果的影响存在争议。本研究旨在探讨内脏肥胖、肌少症或肌少症性肥胖是否会影响同步结直肠癌肝转移患者行肝切除术的预后。
回顾性分析 2013 年 1 月至 2018 年 8 月期间一家单中心数据库中 94 例原发性肝切除术治疗同步结直肠癌肝转移患者的临床资料,包括患者特征和 30 天发病率。采用体层摄影术从 L3 水平的单层面 CT 图像计算体脂和骨骼肌。
59 例(62.8%)患者行小范围肝切除术,35 例(37.2%)行大范围肝切除术。60 例(62.8%)患者术后发生并发症,其中 35 例(Clavien-Dindo 分级 III-V 级)发生严重并发症。术后 30 天死亡率为 0,90 天死亡率为 2.1%。体质指数(BMI)与术后结果无显著相关性(p=1.0)。66 例(70.2%)患者存在内脏肥胖,且与总体并发症和严重并发症发生率显著相关(p=0.002,p=0.012)。34 例(36.2%)患者存在肌少症,但与术后发病率无显著相关性(p=0.461),但肌少症患者的住院时间较长。18 例(19.1%)患者存在肌少症性肥胖,与术后并发症显著相关(p=0.014)。内脏肥胖、肌少症性肥胖和肌少症均被认为是术后总体并发症的显著危险因素。
内脏肥胖、肌少症性肥胖和肌少症是结直肠癌肝转移患者行切除术治疗后总体并发症的独立危险因素。早期识别身体成分的极端情况可能会促使患者进行围手术期干预,从而改善术后结果。