Li Xiaoying, Huang Qian, Lei Yanna, Zheng Xiufeng, Dai Shuang, Leng Weibing, Liu Ming
Department of Abdominal Oncology, West China Hospital, Sichuan University, Chengdu, China.
Ann Transl Med. 2021 Mar;9(6):513. doi: 10.21037/atm-21-434.
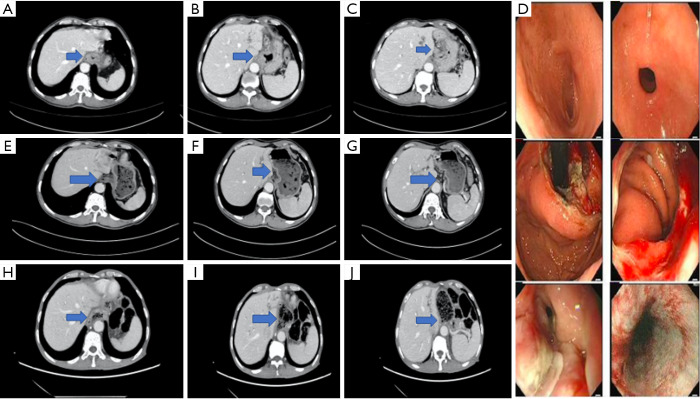
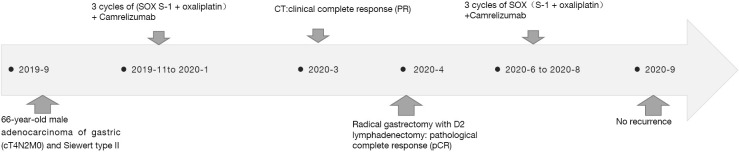
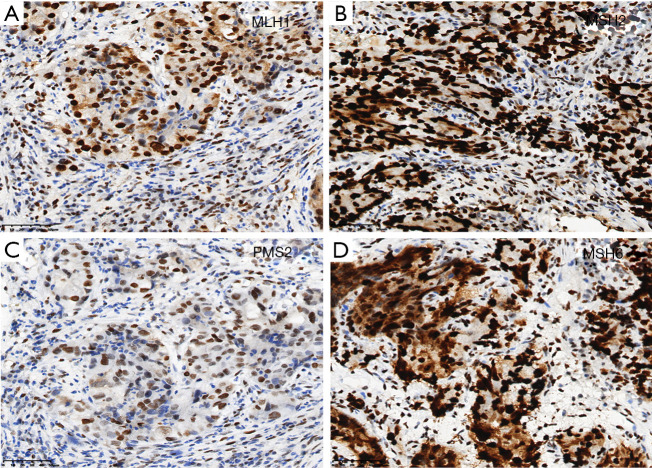
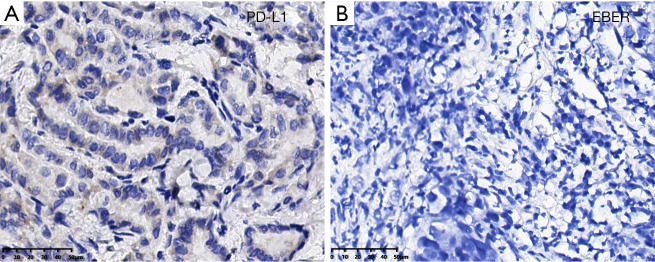
Most gastric cancer and gastroesophageal junction carcinoma (GEJ) patients are already in the advanced stage at the time of diagnosis. Thus, the probability of radical gastrectomy is low, and surgical treatment alone has a poor prognosis due to the high recurrence rate. In order to reduce the recurrence and distant metastasis after surgery, there have been many attempts made to improve the perioperative treatment of advanced localized gastric cancer, but no uniform criteria exist. Over recent years, immunotherapy has revolutionized cancer treatment, and immune checkpoint inhibitors (ICIs) have shown excellent efficacy across various types of tumors, becoming a potential treatment after surgery, chemotherapy, radiotherapy, and targeted therapy. However, the efficacy of single-agent ICIs for gastric cancer is still unsatisfactory. As comprehensive, chemotherapy-based treatment has become the standard care for locally advanced gastric cancer, exploring combination treatment with immune checkpoint inhibitors (ICIs) may be valuable to improving survival outcomes. Here, we report a 66-year-old male with dysphagia diagnosed with GEJ and was defined as clinical stage (cT4N2M0) and Siewert type II, characterized as mismatch repair proficient (pMMR) and programmed cell death ligand-1 (PD-L1) negative; surprisingly, with anti-PD-1 antibody plus SOX (S-1: a combination of tegafur, gimeracil, and oteracil+ oxaliplatin) as perioperative therapy, the patient achieved pathological complete remission (pCR), which indicates that the addition of ICIs to chemotherapy as a perioperative comprehensive treatment might provide a promising strategy option for GEJ. In addition, we review the current status of perioperative comprehensive treatment, in hope that this may provide some reference value for clinical decision-making.
大多数胃癌和胃食管交界癌(GEJ)患者在确诊时已处于晚期。因此,根治性胃切除术的概率较低,且由于复发率高,单纯手术治疗的预后较差。为了降低术后复发和远处转移的风险,人们尝试了多种方法来改进晚期局限性胃癌的围手术期治疗,但尚无统一标准。近年来,免疫疗法彻底改变了癌症治疗方式,免疫检查点抑制剂(ICIs)在各类肿瘤中均显示出优异疗效,成为继手术、化疗、放疗和靶向治疗之后的一种潜在治疗手段。然而,单药ICIs对胃癌的疗效仍不尽人意。由于基于化疗的综合治疗已成为局部晚期胃癌的标准治疗方案,探索免疫检查点抑制剂(ICIs)联合治疗可能对改善生存结局具有重要价值。在此,我们报告一例66岁男性吞咽困难患者,诊断为GEJ,临床分期为(cT4N2M0),Siewert II型,错配修复功能正常(pMMR)且程序性细胞死亡配体-1(PD-L1)阴性;令人惊讶的是,以抗PD-1抗体联合SOX(S-1:替加氟、吉美嘧啶和奥替拉西钾的组合+奥沙利铂)作为围手术期治疗,患者实现了病理完全缓解(pCR),这表明在化疗基础上加用ICIs作为围手术期综合治疗可能为GEJ提供一种有前景的策略选择。此外,我们综述了围手术期综合治疗的现状,希望能为临床决策提供一些参考价值。