Deepak Parakkal, Kim Wooseob, Paley Michael A, Yang Monica, Carvidi Alexander B, El-Qunni Alia A, Haile Alem, Huang Katherine, Kinnett Baylee, Liebeskind Mariel J, Liu Zhuoming, McMorrow Lily E, Paez Diana, Perantie Dana C, Schriefer Rebecca E, Sides Shannon E, Thapa Mahima, Gergely Maté, Abushamma Suha, Klebert Michael, Mitchell Lynne, Nix Darren, Graf Jonathan, Taylor Kimberly E, Chahin Salim, Ciorba Matthew A, Katz Patricia, Matloubian Mehrdad, O'Halloran Jane A, Presti Rachel M, Wu Gregory F, Whelan Sean P J, Buchser William J, Gensler Lianne S, Nakamura Mary C, Ellebedy Ali H, Kim Alfred H J
Inflammatory Bowel Diseases Center, Division of Gastroenterology, Department of Medicine, Washington University School of Medicine, St. Louis, MO, USA.
Division of Immunobiology, Department of Pathology and Immunology, Washington University School of Medicine, St. Louis, MO, USA.
medRxiv. 2021 Apr 9:2021.04.05.21254656. doi: 10.1101/2021.04.05.21254656.
Individuals with chronic inflammatory diseases (CID) are frequently treated with immunosuppressive medications that can increase their risk of severe COVID-19. While novel mRNA-based SARS-CoV-2 vaccination platforms provide robust protection in immunocompetent individuals, the immunogenicity in CID patients on immunosuppression is not well established. Therefore, determining the effectiveness of SARS-CoV-2 vaccines in the setting of immunosuppression is essential to risk-stratify CID patients with impaired protection and provide clinical guidance regarding medication management.
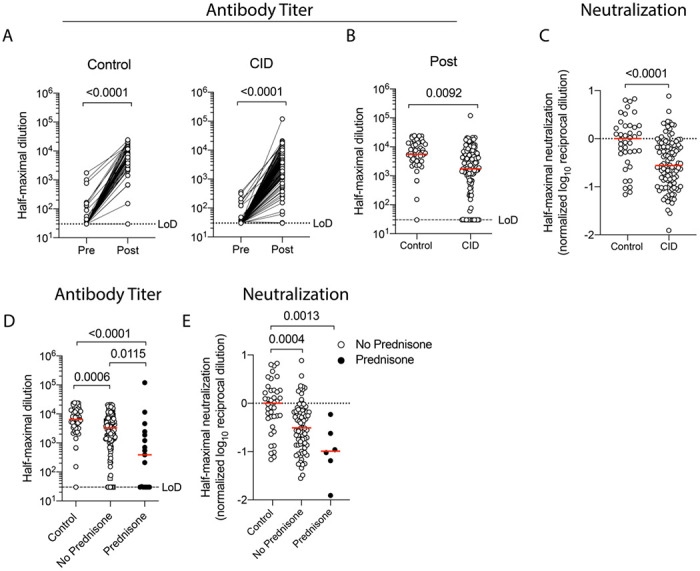
We conducted a prospective assessment of mRNA-based vaccine immunogenicity in 133 adults with CIDs and 53 immunocompetent controls. Blood from participants over 18 years of age was collected before initial immunization and 1-2 weeks after the second immunization. Serum anti-SARS-CoV-2 spike (S) IgG binding, neutralizing antibody titers, and circulating S-specific plasmablasts were quantified to assess the magnitude and quality of the humoral response following vaccination.
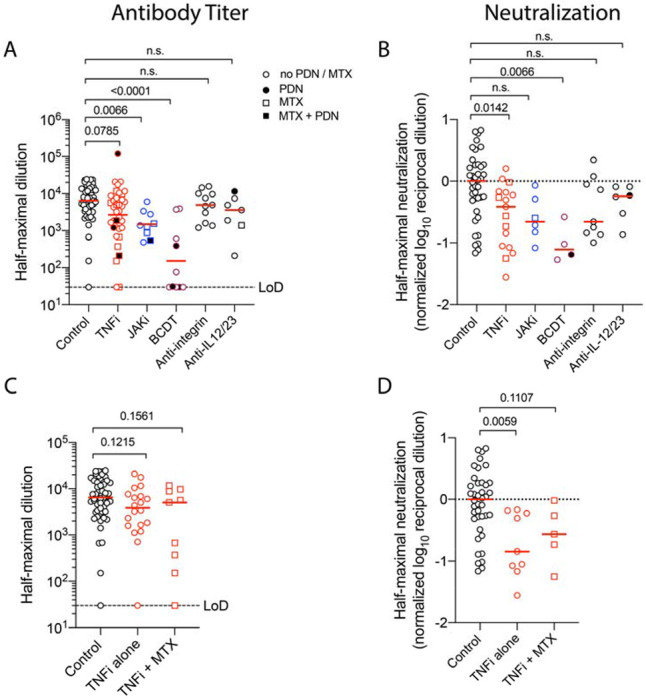
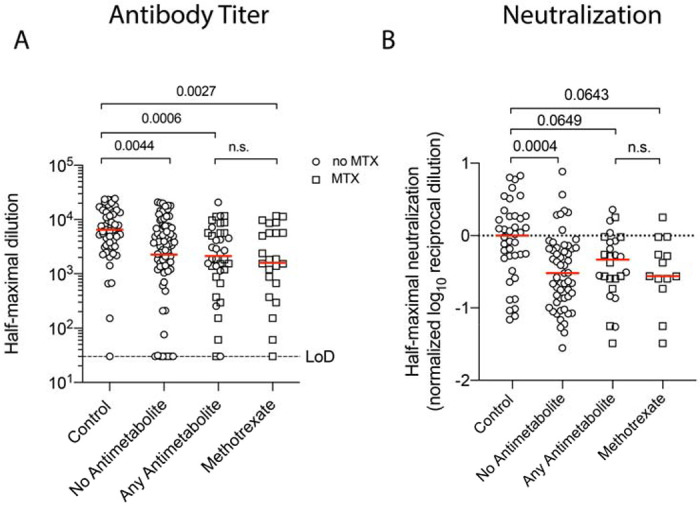
Compared to immunocompetent controls, a three-fold reduction in anti-S IgG titers (P=0.009) and SARS-CoV-2 neutralization (p<0.0001) were observed in CID patients. B cell depletion and glucocorticoids exerted the strongest effect with a 36- and 10-fold reduction in humoral responses, respectively (p<0.0001). Janus kinase inhibitors and antimetabolites, including methotrexate, also blunted antibody titers in multivariate regression analysis (P<0.0001, P=0.0023, respectively). Other targeted therapies, such as TNF inhibitors, IL-12/23 inhibitors, and integrin inhibitors, had only modest impacts on antibody formation and neutralization.
CID patients treated with immunosuppressive therapies exhibit impaired SARS-CoV-2 vaccine-induced immunity, with glucocorticoids and B cell depletion therapy more severely impeding optimal responses.
患有慢性炎症性疾病(CID)的个体经常接受免疫抑制药物治疗,这会增加他们患重症 COVID-19 的风险。虽然新型基于 mRNA 的 SARS-CoV-2 疫苗平台在免疫功能正常的个体中提供了强大的保护,但免疫抑制状态下 CID 患者的免疫原性尚未明确。因此,确定 SARS-CoV-2 疫苗在免疫抑制情况下的有效性对于对保护功能受损的 CID 患者进行风险分层以及提供有关药物管理的临床指导至关重要。
我们对 133 名患有 CID 的成年人和 53 名免疫功能正常的对照者进行了基于 mRNA 的疫苗免疫原性的前瞻性评估。在初次免疫前和第二次免疫后 1-2 周收集 18 岁以上参与者的血液。对血清抗 SARS-CoV-2 刺突(S)IgG 结合、中和抗体滴度和循环 S 特异性浆母细胞进行定量,以评估疫苗接种后体液反应的强度和质量。
与免疫功能正常的对照者相比,CID 患者的抗 S IgG 滴度(P = 0.009)和 SARS-CoV-2 中和能力(p < 0.0001)降低了三倍。B 细胞耗竭和糖皮质激素的影响最强,体液反应分别降低了 36 倍和 10 倍(p < 0.0001)。在多变量回归分析中,包括甲氨蝶呤在内的 Janus 激酶抑制剂和抗代谢物也使抗体滴度降低(分别为 P < 0.0001,P = 0.0023)。其他靶向治疗,如 TNF 抑制剂、IL-12/23 抑制剂和整合素抑制剂,对抗体形成和中和的影响较小。
接受免疫抑制治疗的 CID 患者表现出 SARS-CoV-2 疫苗诱导的免疫功能受损,糖皮质激素和 B 细胞耗竭疗法更严重地阻碍了最佳反应。