Epidemiology and Health Care Research, German Rheumatism Research Center (DRFZ Berlin), Berlin, Germany.
Division of Rheumatology, Department of Medicine, University of California, San Francisco, CA, USA.
Ann Rheum Dis. 2021 Jul;80(7):930-942. doi: 10.1136/annrheumdis-2020-219498. Epub 2021 Jan 27.
To determine factors associated with COVID-19-related death in people with rheumatic diseases.
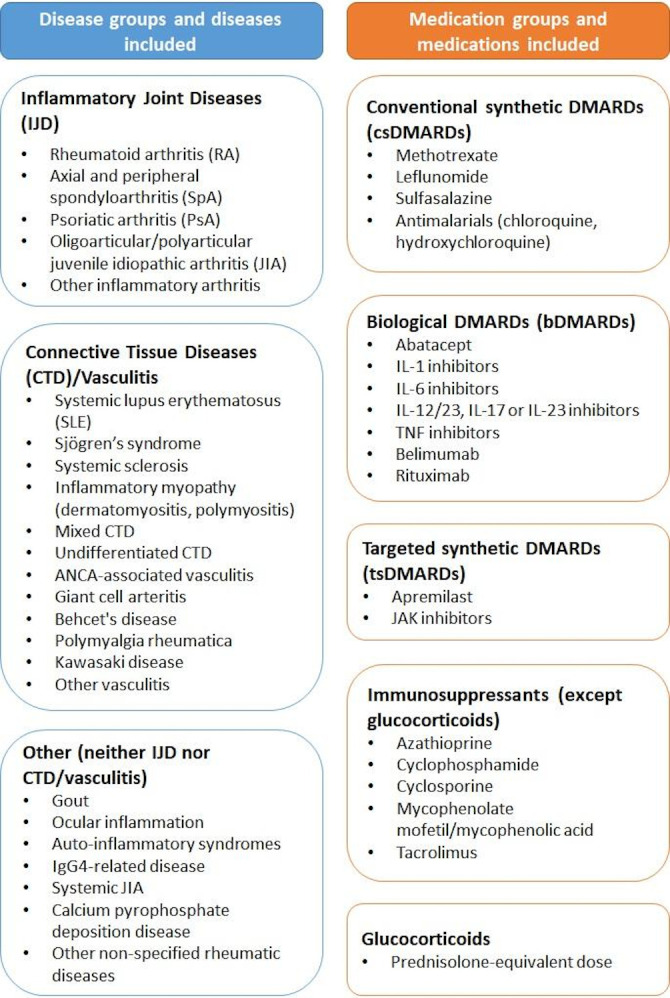
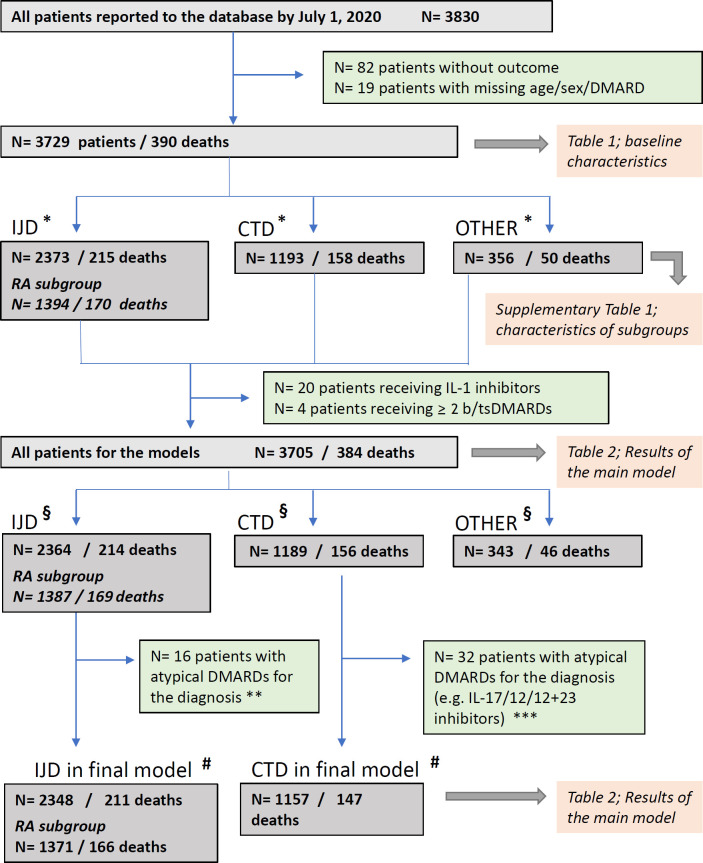
Physician-reported registry of adults with rheumatic disease and confirmed or presumptive COVID-19 (from 24 March to 1 July 2020). The primary outcome was COVID-19-related death. Age, sex, smoking status, comorbidities, rheumatic disease diagnosis, disease activity and medications were included as covariates in multivariable logistic regression models. Analyses were further stratified according to rheumatic disease category.
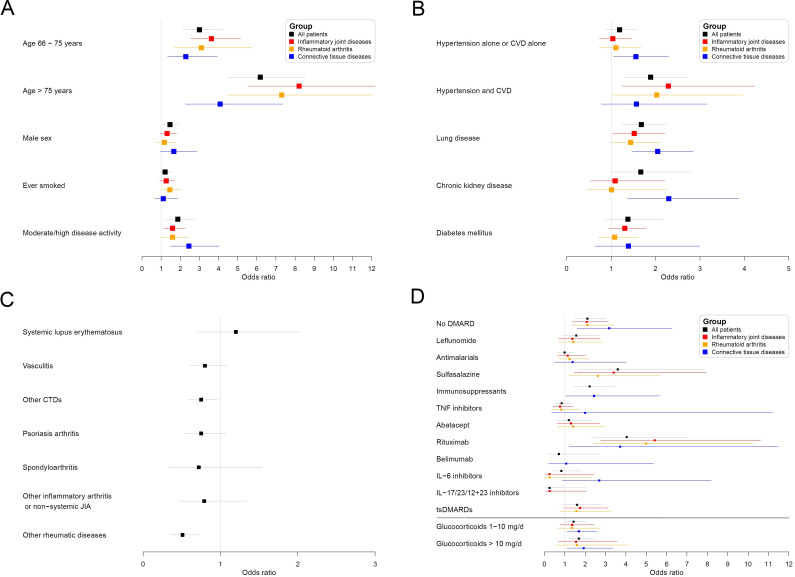
Of 3729 patients (mean age 57 years, 68% female), 390 (10.5%) died. Independent factors associated with COVID-19-related death were age (66-75 years: OR 3.00, 95% CI 2.13 to 4.22; >75 years: 6.18, 4.47 to 8.53; both vs ≤65 years), male sex (1.46, 1.11 to 1.91), hypertension combined with cardiovascular disease (1.89, 1.31 to 2.73), chronic lung disease (1.68, 1.26 to 2.25) and prednisolone-equivalent dosage >10 mg/day (1.69, 1.18 to 2.41; vs no glucocorticoid intake). Moderate/high disease activity (vs remission/low disease activity) was associated with higher odds of death (1.87, 1.27 to 2.77). Rituximab (4.04, 2.32 to 7.03), sulfasalazine (3.60, 1.66 to 7.78), immunosuppressants (azathioprine, cyclophosphamide, ciclosporin, mycophenolate or tacrolimus: 2.22, 1.43 to 3.46) and not receiving any disease-modifying anti-rheumatic drug (DMARD) (2.11, 1.48 to 3.01) were associated with higher odds of death, compared with methotrexate monotherapy. Other synthetic/biological DMARDs were not associated with COVID-19-related death.
Among people with rheumatic disease, COVID-19-related death was associated with known general factors (older age, male sex and specific comorbidities) and disease-specific factors (disease activity and specific medications). The association with moderate/high disease activity highlights the importance of adequate disease control with DMARDs, preferably without increasing glucocorticoid dosages. Caution may be required with rituximab, sulfasalazine and some immunosuppressants.
确定与风湿性疾病患者 COVID-19 相关死亡相关的因素。
医生报告的成年风湿性疾病患者登记处和确诊或疑似 COVID-19(2020 年 3 月 24 日至 7 月 1 日)。主要结局是 COVID-19 相关死亡。年龄、性别、吸烟状况、合并症、风湿性疾病诊断、疾病活动度和药物治疗被纳入多变量逻辑回归模型中的协变量。根据风湿性疾病类别进一步分层分析。
在 3729 名患者(平均年龄 57 岁,68%为女性)中,有 390 人(10.5%)死亡。与 COVID-19 相关死亡相关的独立因素包括年龄(66-75 岁:OR 3.00,95%CI 2.13 至 4.22;>75 岁:6.18,4.47 至 8.53;均与≤65 岁相比)、男性(1.46,1.11 至 1.91)、高血压合并心血管疾病(1.89,1.31 至 2.73)、慢性肺部疾病(1.68,1.26 至 2.25)和泼尼松等效剂量>10mg/天(1.69,1.18 至 2.41;与无糖皮质激素摄入相比)。中度/高度疾病活动度(与缓解/低度疾病活动度相比)与死亡几率更高相关(1.87,1.27 至 2.77)。利妥昔单抗(4.04,2.32 至 7.03)、柳氮磺胺吡啶(3.60,1.66 至 7.78)、免疫抑制剂(硫唑嘌呤、环磷酰胺、环孢素、霉酚酸酯或他克莫司:2.22,1.43 至 3.46)和未接受任何改善病情的抗风湿药物(DMARD)(2.11,1.48 至 3.01)与死亡几率更高相关,而与甲氨蝶呤单药治疗相比。其他合成/生物 DMARD 与 COVID-19 相关死亡无关。
在风湿性疾病患者中,COVID-19 相关死亡与已知的一般因素(年龄较大、男性和特定合并症)和疾病特异性因素(疾病活动度和特定药物)相关。与中度/高度疾病活动度相关强调了使用 DMARD 进行充分疾病控制的重要性,最好不增加糖皮质激素剂量。可能需要谨慎使用利妥昔单抗、柳氮磺胺吡啶和一些免疫抑制剂。