Paediatric Intensive Care Unit, Department of Paediatrics, Sapienza University of Rome, Rome, Italy.
Medical Engineering Laboratory, Department of Civil Engineering and Computer Science Engineering, University of Rome "Tor Vergata", Rome, Italy.
Paediatr Anaesth. 2021 Jul;31(7):809-819. doi: 10.1111/pan.14194. Epub 2021 May 6.
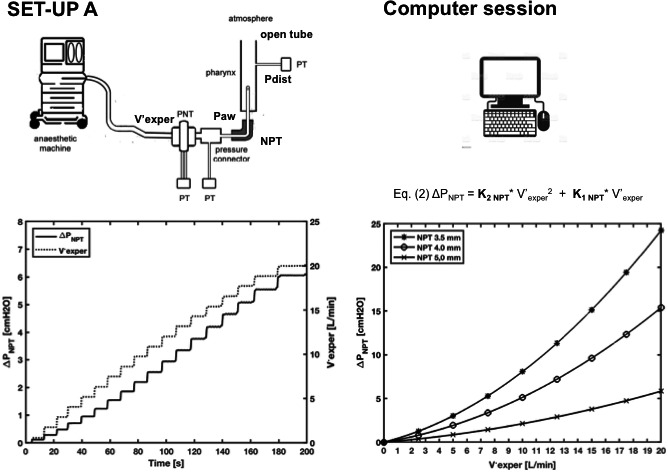
Nasopharyngeal tubes are useful in pediatric anesthesia for insufflating oxygen and anesthetics. During nasopharyngeal tube-anesthesia, gas insufflation provides some positive oropharyngeal pressure that differs from the proximal airway pressure owing to the flow-dependent pressure drop across the nasopharyngeal tube (ΔP ).
This study aimed to investigate whether ΔP could be used for calculating oropharyngeal pressure during nasopharyngeal tube-assisted anesthesia.
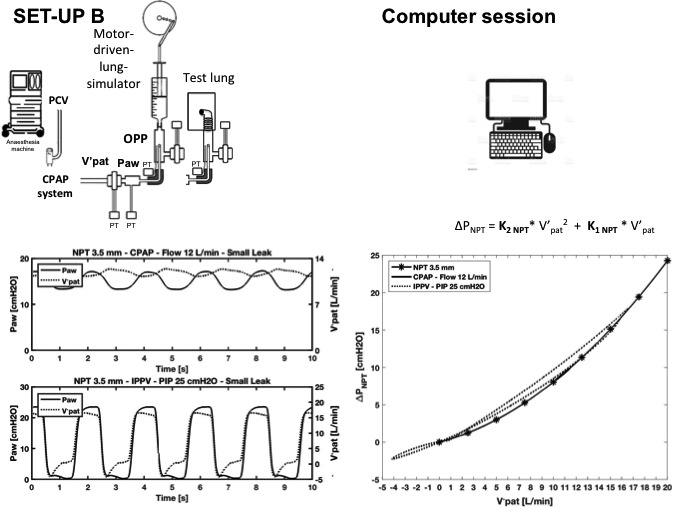
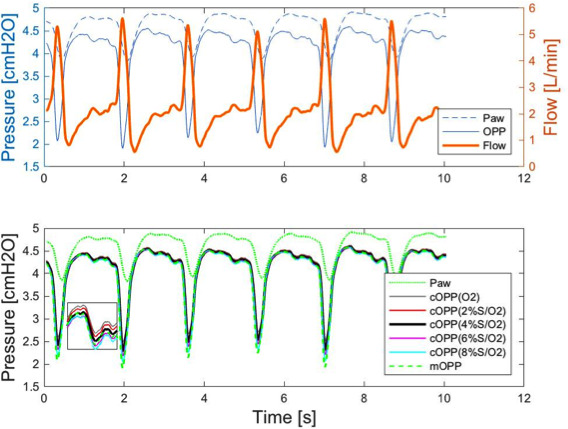
In a physical model of nasopharyngeal tube-anesthesia, using Rohrer's equation, we calculated ΔP for three nasopharyngeal tubes (3.5, 4.0, and 5.0 mm inner diameter) under oxygen and several sevoflurane in oxygen combinations in two ventilatory scenarios (continuous positive airway pressure and intermittent positive pressure ventilation). We then calculated oropharyngeal pressure as proximal airway pressure minus ΔP . Calculated and measured oropharyngeal pressure couples of values were compared with the root mean square deviation to assess accuracy. We also investigated whether oropharyngeal pressure accuracy depends on the nasopharyngeal tube diameter, flow rate, gas composition, and leak size. Using ΔP charts, we tested whether ΔP calculation was feasible in clinical practice.
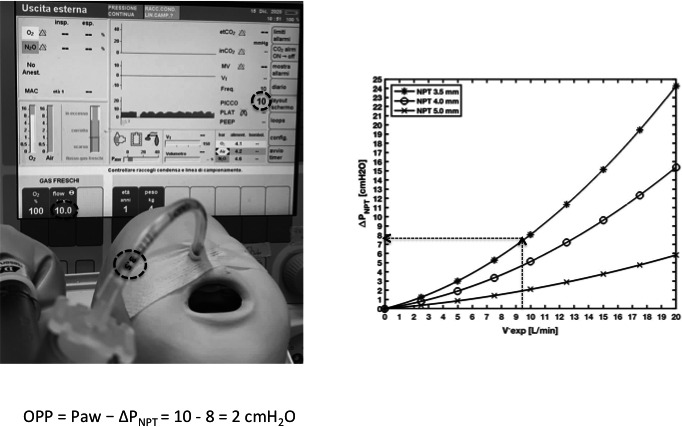
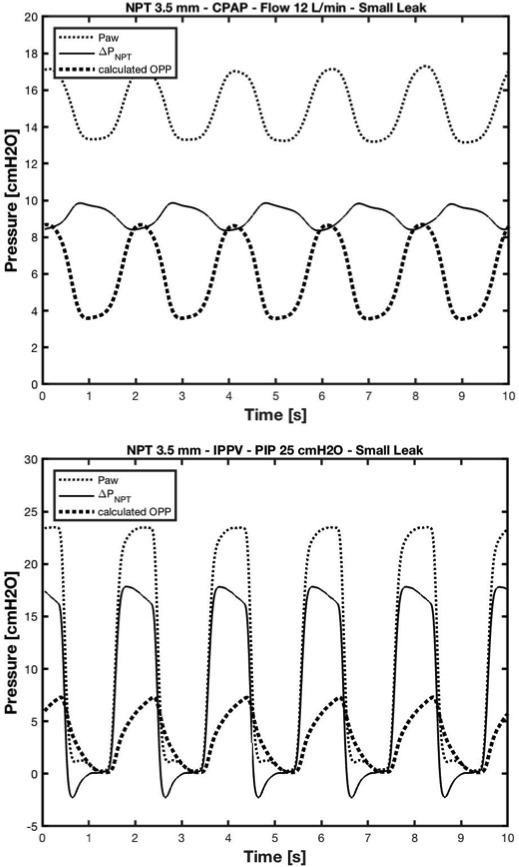
When we tested small-diameter nasopharyngeal tubes at high-flow or high-peak inspiratory pressure, proximal airway pressure measurements markedly overestimated oropharyngeal pressure. Comparing measured and calculated maximum and minimum oropharyngeal pressure couples yielded root mean square deviations less than 0.5 cmH O regardless of ventilatory modality, nasopharyngeal tube diameter, flow rate, gas composition, and leak size.
During nasopharyngeal tube-assisted anesthesia, proximal airway pressure readings on the anesthetic monitoring machine overestimate oropharyngeal pressure especially for smaller-diameter nasopharyngeal tubes and higher flow, and to a lesser extent for large leaks. Given the importance of calculating oropharyngeal pressure in guiding nasopharyngeal tube ventilation in clinical practice, we propose an accurate calculation using Rohrer's equation method, or approximating oropharyngeal pressure from flow and pressure readings on the anesthetic machine using the ΔP charts.
在小儿麻醉中,鼻咽通气管可用于输送氧气和麻醉剂。在经鼻咽通气管麻醉期间,由于通过鼻咽通气管的气流依赖性压力降,气体输送会提供一些正压口咽压力,这与近端气道压力不同(ΔP)。
本研究旨在探讨在经鼻咽通气管辅助麻醉期间,ΔP 是否可用于计算口咽压力。
在鼻咽通气管麻醉的物理模型中,使用 Rohrer 方程,我们计算了三种内径(3.5、4.0 和 5.0 毫米)的鼻咽通气管在两种通气模式(持续气道正压通气和间歇正压通气)下,在氧气和几种七氟醚与氧气组合下的ΔP。然后,我们将口咽压力计算为近端气道压力减去ΔP。比较计算和测量的口咽压力对值与均方根偏差,以评估准确性。我们还研究了口咽压力的准确性是否取决于鼻咽通气管的直径、流量、气体组成和泄漏大小。使用ΔP 图表,我们测试了在临床实践中计算ΔP 是否可行。
当我们在高流量或高吸气峰压下测试小直径鼻咽通气管时,近端气道压力测量值显著高估了口咽压力。比较测量和计算的最大和最小口咽压力对值,均方根偏差小于 0.5 cmH2O,无论通气方式、鼻咽通气管直径、流量、气体组成和泄漏大小如何。
在经鼻咽通气管辅助麻醉期间,麻醉监测仪上的近端气道压力读数会高估口咽压力,尤其是对于较小直径的鼻咽通气管和更高的流量,并且在较小程度上对于较大的泄漏。鉴于在临床实践中计算口咽压力对口咽通气管通气的指导意义重大,我们建议使用 Rohrer 方程方法进行准确计算,或者使用麻醉机上的流量和压力读数,通过ΔP 图表近似计算口咽压力。