Division of Medical Oncology, Memorial Hospital, Antalya, Turkey.
Genekor Medical S.A, Athens, Greece.
BMC Med Genomics. 2021 Apr 14;14(1):105. doi: 10.1186/s12920-021-00952-9.
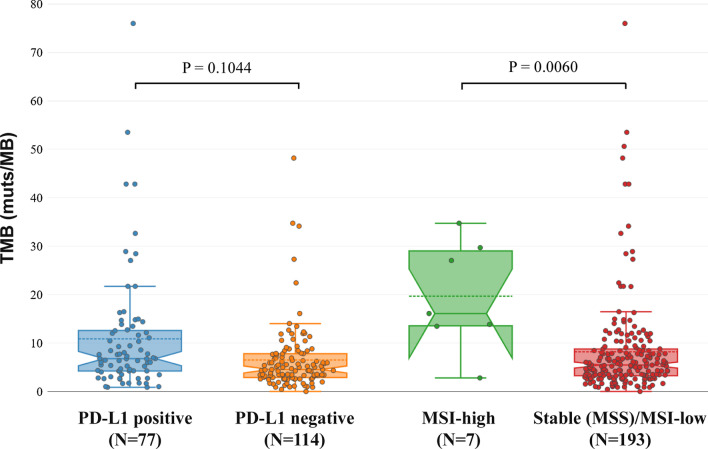
Tumor molecular profile analysis by Next Generation Sequencing technology is currently widely applied in clinical practice and has enabled the detection of predictive biomarkers of response to targeted treatment. In parallel with targeted therapies, immunotherapies are also evolving, revolutionizing cancer therapy, with Programmed Death-ligand 1 (PD-L1), Microsatellite instability (MSI), and Tumor Mutational Burden (TMB) analysis being the biomarkers employed most commonly.
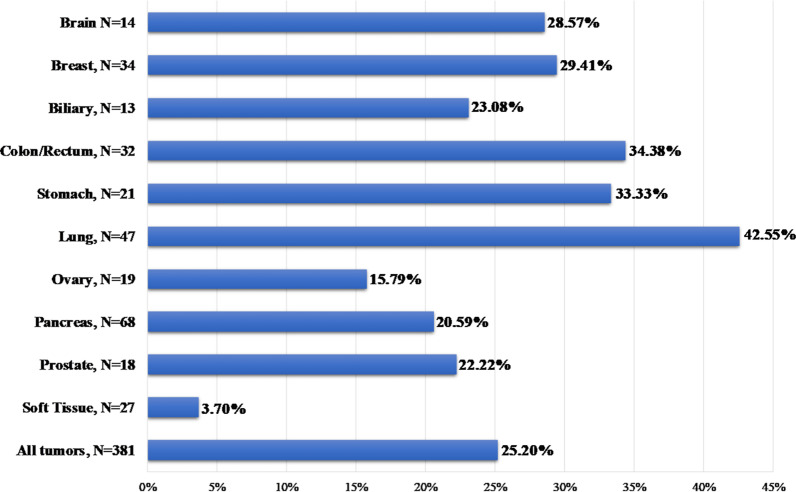
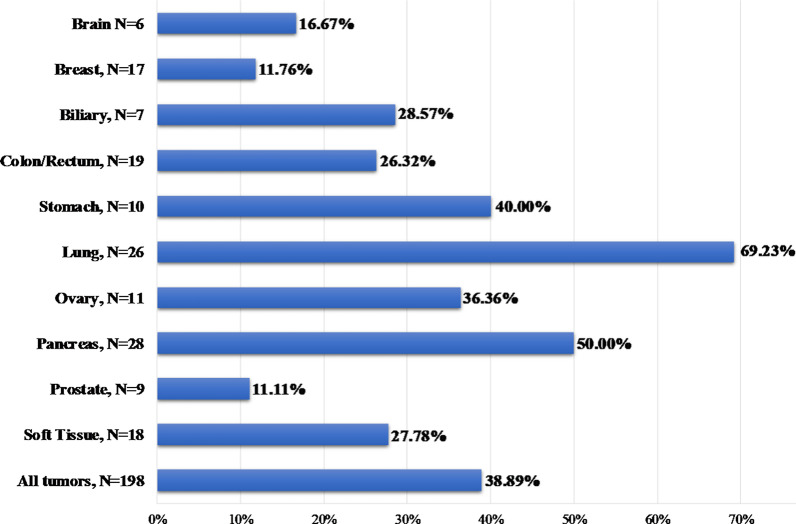
In the present study, tumor molecular profile analysis was performed using a 161 gene NGS panel, containing the majority of clinically significant genes for cancer treatment selection. A variety of tumor types have been analyzed, including aggressive and hard to treat cancers such as pancreatic cancer. Besides, the clinical utility of immunotherapy biomarkers (TMB, MSI, PD-L1), was also studied.
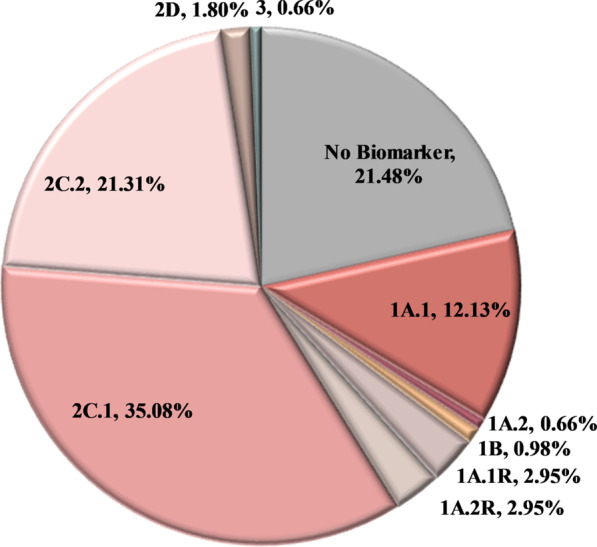
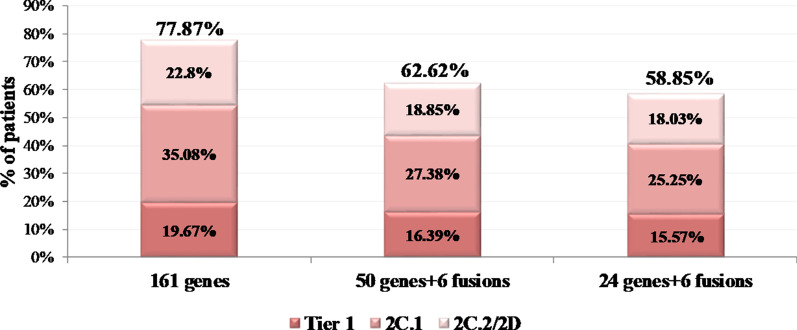
Molecular profile analysis was conducted in 610 cancer patients, while in 393 of them a at least one biomarker for immunotherapy response was requested. An actionable alteration was detected in 77.87% of the patients. 54.75% of them received information related to on-label or off-label treatment (Tiers 1A.1, 1A.2, 2B, and 2C.1) and 21.31% received a variant that could be used for clinical trial inclusion. The addition to immunotherapy biomarker to targeted biomarkers' analysis in 191 cases increased the number of patients with an on-label treatment recommendation by 22.92%, while an option for on-label or off-label treatment was provided in 71.35% of the cases.
Tumor molecular profile analysis using NGS is a first-tier method for a variety of tumor types and provides important information for decision making in the treatment of cancer patients. Importantly, simultaneous analysis for targeted therapy and immunotherapy biomarkers could lead to better tumor characterization and offer actionable information in the majority of patients. Furthermore, our data suggest that one in two patients may be eligible for on-label ICI treatment based on biomarker analysis. However, appropriate interpretation of results from such analysis is essential for implementation in clinical practice and accurate refinement of treatment strategy.
下一代测序技术的肿瘤分子谱分析目前在临床实践中得到广泛应用,能够检测出针对靶向治疗反应的预测生物标志物。随着靶向治疗的发展,免疫疗法也在不断发展,彻底改变了癌症治疗,程序性死亡配体 1(PD-L1)、微卫星不稳定性(MSI)和肿瘤突变负荷(TMB)分析是最常用的生物标志物。
本研究采用包含大多数癌症治疗选择有意义的基因的 161 基因 NGS 面板进行肿瘤分子谱分析。分析了多种肿瘤类型,包括胰腺癌等侵袭性和难以治疗的癌症。此外,还研究了免疫治疗生物标志物(TMB、MSI、PD-L1)的临床应用价值。
对 610 例癌症患者进行了分子谱分析,其中 393 例患者请求进行免疫治疗反应的至少一个生物标志物分析。77.87%的患者检测到可采取的改变。其中 54.75%的患者获得了与标签内或标签外治疗相关的信息(1A.1、1A.2、2B 和 2C.1 层),21.31%的患者获得了可用于临床试验纳入的变异。在 191 例患者中增加免疫治疗生物标志物与靶向生物标志物分析相结合,使具有标签内治疗推荐的患者数量增加了 22.92%,同时 71.35%的患者有标签内或标签外治疗的选择。
使用 NGS 的肿瘤分子谱分析是多种肿瘤类型的一线方法,为癌症患者的治疗决策提供了重要信息。重要的是,同时进行靶向治疗和免疫治疗生物标志物分析可以更好地对肿瘤进行特征描述,并为大多数患者提供可采取的信息。此外,我们的数据表明,基于生物标志物分析,每两名患者中就有一名可能有资格接受标签内 ICI 治疗。然而,对于实施临床实践和准确调整治疗策略,适当解释此类分析的结果至关重要。